Orthognathic Surgery: When the Jaws Themselves Are Out of Place
Years of braces, and the bite still doesn’t close in front. Or the lower jaw sits so far back that the chin almost disappears, or so far forward that the lower teeth lead. Maybe one side of the face is fuller, the midlines don’t line up, and the smile tilts. The teeth have been moved every way they can be moved — and the problem is still there, because the problem was never really the teeth.
It’s the jaws. Orthognathic surgery — corrective jaw surgery — repositions the upper jaw, lower jaw, or both so they meet correctly and the face is balanced. It is the answer when the skeleton, not the dentition, is the source of the problem.
The Real Problem: A Skeletal Mismatch, Not a Tooth Problem
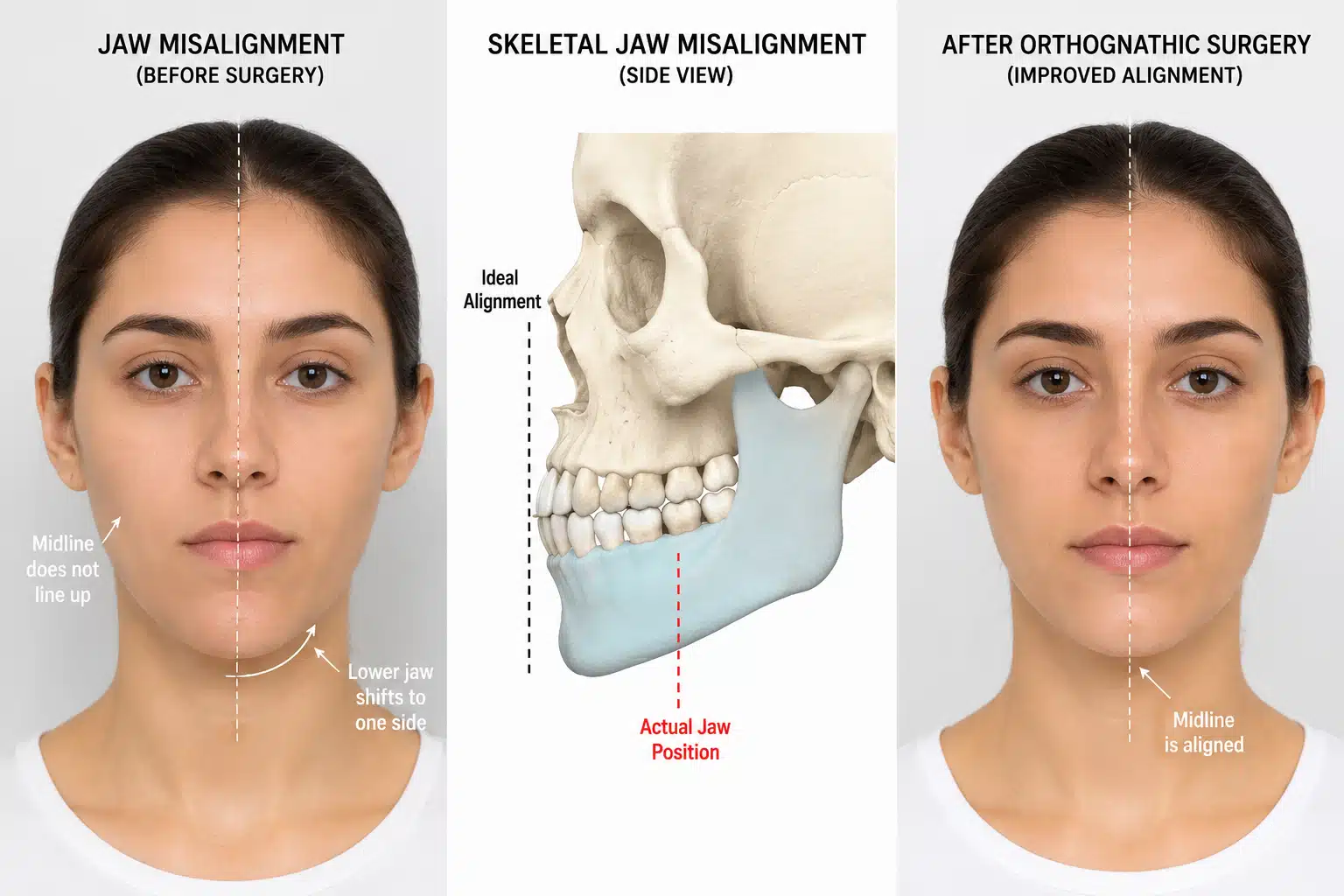
Teeth sit in two movable platforms: the upper jaw (maxilla) and lower jaw (mandible). When those platforms are the wrong size, shape, or position relative to each other, no amount of tooth movement makes them fit. The result shows up as an underbite, a protruding or recessed jaw, an anterior open bite where the front teeth never touch, crowding the airway, or facial asymmetry. Patients often arrive having been treated for years as though it were a tooth problem.
Sometimes the mismatch is a stable developmental difference. Other times it is being actively driven — by an overgrowing condyle in condylar hyperplasia, or by a dissolving one in idiopathic condylar resorption. Telling stable from progressive is critical, because operating on a moving target relapses.

What an Experienced Surgeon Brings to the Decision
The value of a focused practice is separating a stable skeletal difference from one still being driven by a growth or joint problem, and planning the jaw movements so the bite, the face, the joints, and the airway all end up working together.
Dr. Larry Wolford has more than four decades of experience in orthognathic surgery and has published extensively on jaw repositioning, including its interaction with the temporomandibular joints and the airway. When a joint problem underlies the asymmetry, he addresses the joint and the jaws in a coordinated plan — sometimes in a single operation — rather than correcting the bite over an unstable joint. That experience doesn’t change your anatomy, but it changes how accurately the cause is identified and how stable the result tends to be.
Key Takeaways
- Orthognathic surgery corrects the jaws themselves, not just the teeth — for problems braces alone cannot fix.
- It treats underbites, open bites, recessed or protruding jaws, facial asymmetry, and some airway problems.
- It is usually combined with orthodontics before and after surgery, planned jointly from the start.
- Asymmetry that keeps worsening can signal an active growth or joint problem that must be addressed first.
- The same jaw movements can be used to enlarge the airway in obstructive sleep apnea.
- Goals are a functional, stable bite and a balanced face; outcomes vary and are never guaranteed.
How the Decision Is Actually Made
Here is the reasoning behind that answer.
The source of the problem is identified. Records, photos over time, and 3D imaging determine whether the jaws are simply mismatched or whether the mismatch is progressing — which points to a growth or joint cause.
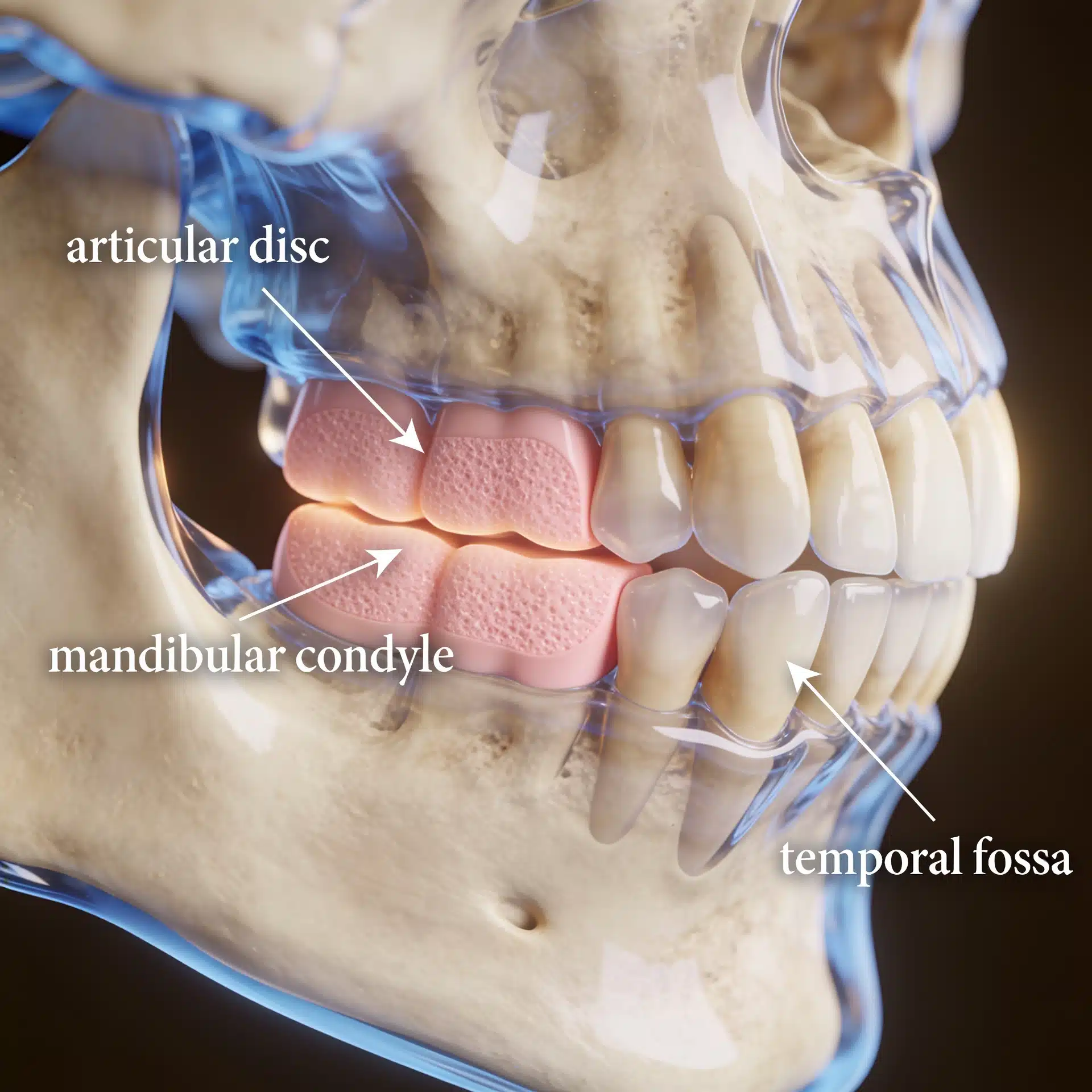
The joints are evaluated. Because the jaws hinge on the temporomandibular joints, an MRI evaluation of the TMJ may be used to confirm the joints are healthy enough to support the planned movements, or to plan disc repositioning or joint reconstruction when they aren’t.
Orthodontics and surgery are coordinated. The teeth are aligned within each jaw so that, once the jaws are repositioned, the bite fits — which is why orthodontist and surgeon plan together from the beginning.

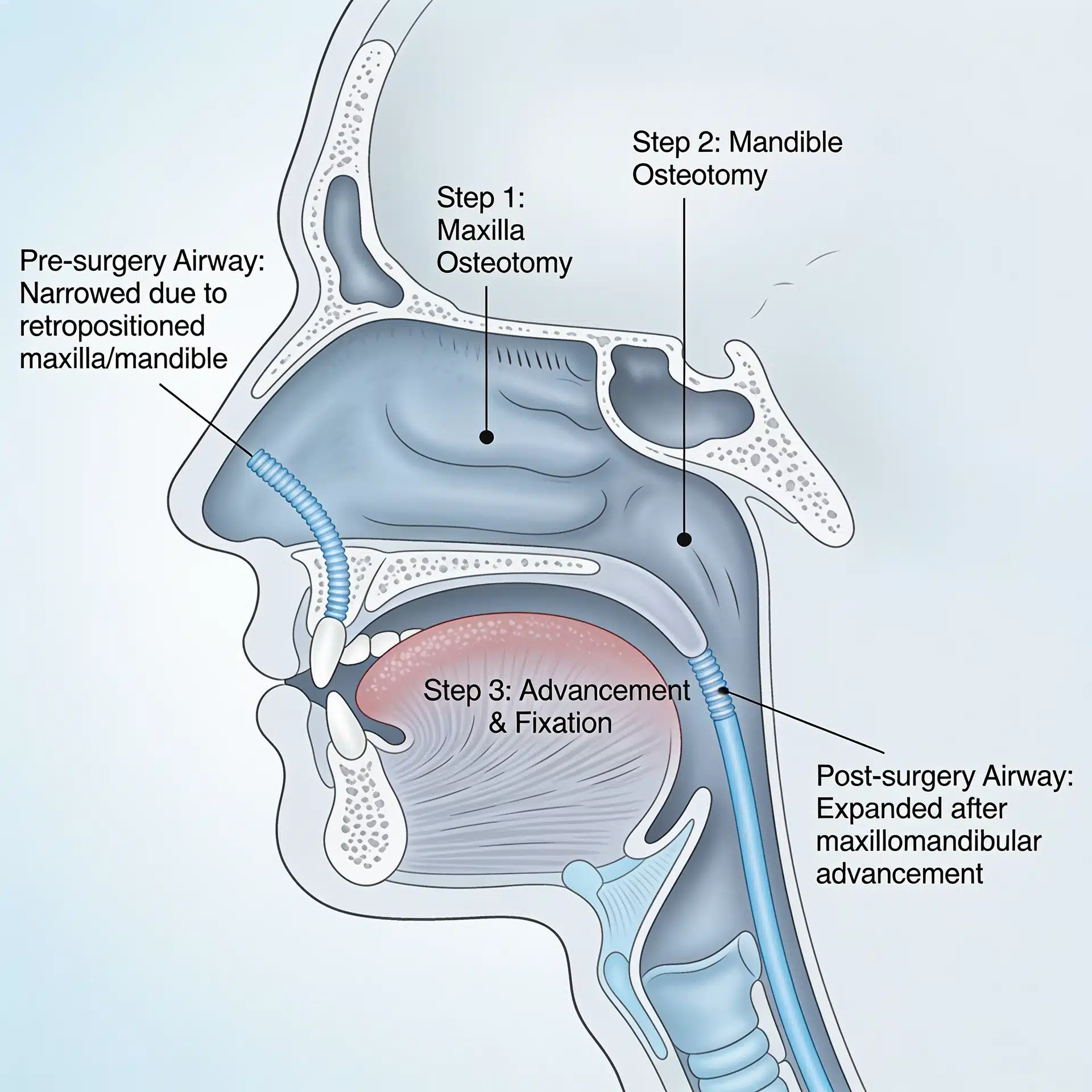
The airway is considered. When breathing or sleep is a concern, the jaw movements can be planned to enlarge the airway, the principle behind maxillomandibular advancement.
Success is defined honestly. Realistic goals are a functional, stable bite, a balanced face, and protected joints and airway — not a guarantee of perfect symmetry. Every surgery carries risk, and a candid discussion of those risks is part of informed consent.
Where This Care Happens
Dr. Wolford’s practice is located on the campus of Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 — minutes from downtown Dallas and accessible from across the Dallas–Fort Worth metroplex. Valet parking is available, with self-parking in the adjacent building.
Patients travel to Dallas from across the country and internationally for complex jaw correction, particularly when a joint problem is involved. All procedures for both current and new patients are performed exclusively at the Dallas office. Out-of-town patients can review what to bring — including orthodontic records, imaging, and photos over time — on the patient information page.
Frequently Asked Questions
How do I know if I need jaw surgery and not just braces?
Braces correct the position of teeth within the jaws. When the jaws themselves are the wrong size, shape, or position — an underbite, an open bite that won’t close, a receded lower jaw, or facial asymmetry — moving the teeth alone can’t fix it. A combined orthodontic and surgical evaluation determines which problem you have.
Is orthognathic surgery cosmetic?
It is primarily functional — correcting how the jaws meet so you can bite, chew, and sometimes breathe properly. Because the jaws also shape the face, it typically improves facial balance as a result, but the core purpose is function and stability.
Does the surgery involve braces too?
Usually. Orthodontics before and after surgery aligns the teeth within each jaw so the bite fits once the jaws are repositioned. The orthodontist and surgeon coordinate the plan from the start.
Can it help my breathing or sleep apnea?
Sometimes. Repositioning the jaws can enlarge the airway, which is the basis of maxillomandibular advancement for obstructive sleep apnea. When breathing is a concern, the airway is planned along with the bite.
What if my asymmetry keeps getting worse?
Progressive asymmetry can signal an active jaw-growth or joint problem — such as condylar hyperplasia or condylar resorption — rather than a stable difference. The underlying cause must be evaluated and addressed before or with the jaw surgery, or the correction tends to relapse.
Related Reading on This Site
Authoritative Resources (External)
These independent, non-commercial sources offer further patient education:
- American Association of Oral and Maxillofacial Surgeons — corrective jaw (orthognathic) surgery overview
- National Institute of Dental and Craniofacial Research (NIH) — jaw-joint context and TMD
- MedlinePlus (U.S. National Library of Medicine) — overview of malocclusion of the teeth
A note on patient stories: Any patient example used in marketing for this practice should be either fully de-identified or used only with written patient authorization, consistent with HIPAA. Because these conditions often affect minors, particular care should be taken with consent and de-identification. The scenarios described in this article are general and composite, not specific patients. This article is educational and is not a substitute for individualized medical advice.