Articular Disc Repositioning: Putting the Jaw Joint’s Cushion Back Where It Belongs
It often begins as a click. The jaw pops opening a sandwich, then pops again closing. For a while it’s just a noise. Then the noise turns into a catch, the catch into a morning when the mouth won’t open all the way, and eventually into a joint that aches and grinds. Somewhere in that progression, a small cushion inside the joint has slipped out of place — and stayed there.
That cushion is the articular disc, and where it sits matters enormously. Disc repositioning is the surgery that returns it to its proper place and holds it there. The goal isn’t only to quiet a click; it’s to stop a slow chain of damage before the joint itself gives way.
The Real Problem: A Cushion That Slipped Forward
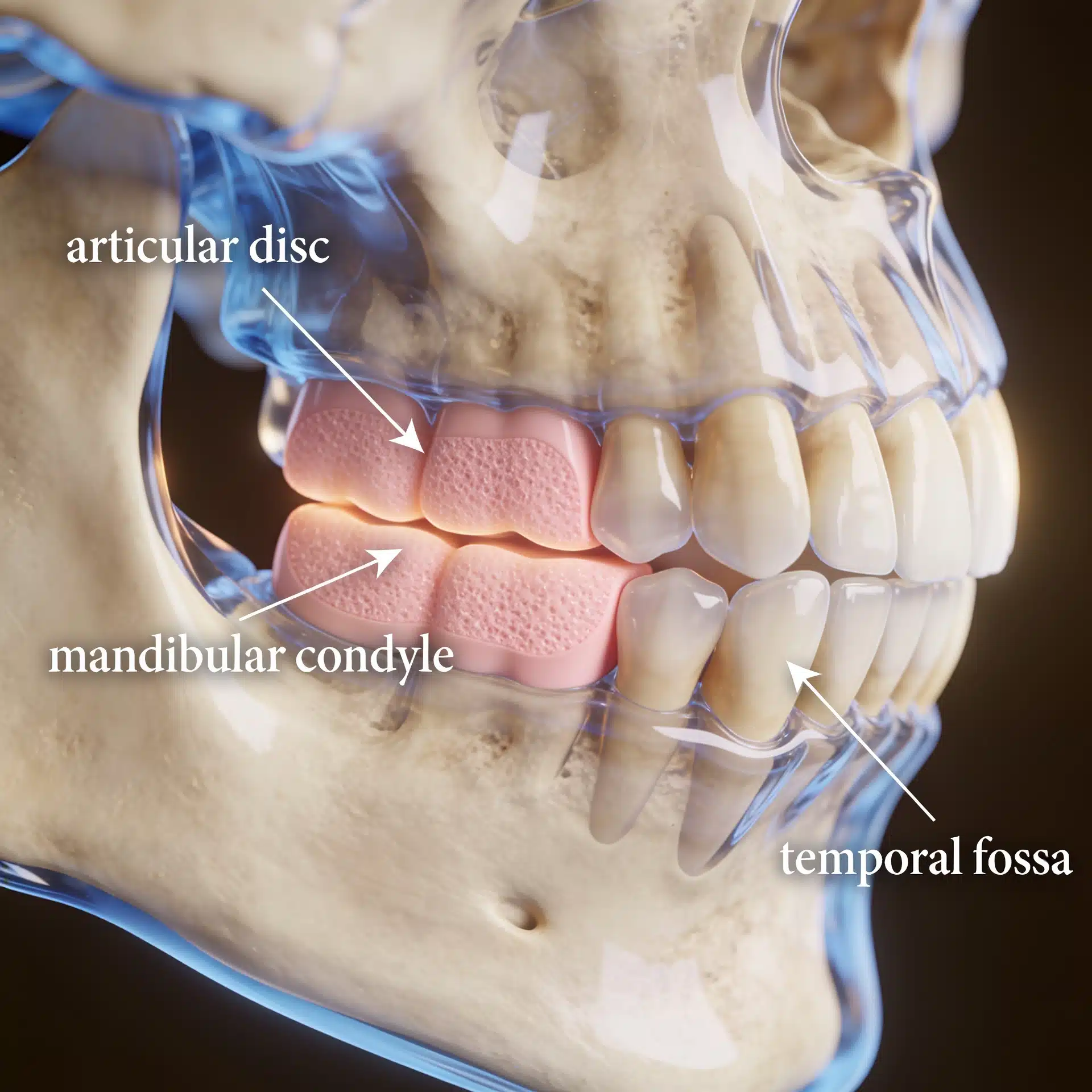
The articular disc is a small pad of tissue that rides between the condyle and the skull base, gliding with the jaw so bone never grinds on bone. When it displaces — usually forward — the smooth glide is lost. Early on the disc may snap back into place with a click. Later it can block the joint entirely (a closed lock), limiting how far the mouth opens. Over time, a chronically displaced disc exposes the joint surfaces to wear and can contribute to degeneration and even condylar resorption.
This is the most common form of internal derangement behind TMJ dysfunction. Not every clicking joint needs surgery — many are managed conservatively. But when the displacement is painful, progressive, or part of a larger skeletal problem, leaving the disc out of place lets the damage continue.

What an Experienced Surgeon Brings to the Decision
The judgment here is knowing which joints will benefit from repositioning, confirming the disc is salvageable, and securing it so it actually stays put — because a disc that simply drifts forward again has gained nothing.
Dr. Larry Wolford has more than four decades of experience in TMJ surgery and has published extensively on disc repositioning using a small bone anchor (the Mitek anchor technique) to stabilize the repositioned disc over the condyle. When a misaligned bite or facial asymmetry is part of the picture, he frequently stabilizes the joint and performs corrective jaw surgery in one coordinated operation. That experience doesn’t change your anatomy, but it changes how reliably the disc is stabilized and how completely the underlying joint problem is addressed.
Key Takeaways
- The articular disc is the jaw joint’s cushion; when it slips forward, the joint clicks, can lock, and is exposed to wear.
- Disc displacement is the most common internal derangement behind TMJ dysfunction.
- Not every clicking joint needs surgery — repositioning is for symptomatic, progressive, or reconstructive cases.
- The Mitek anchor technique returns the disc to position and secures it so it does not drift forward again.
- Stabilizing the disc is intended to protect the joint surfaces and slow degeneration.
- It may be done alone or combined with corrective jaw surgery; outcomes vary and are never guaranteed.
How the Decision Is Actually Made
Here is the reasoning behind that answer.
Imaging confirms the disc is displaced and salvageable. An MRI evaluation of the TMJ shows the disc’s position and condition. A disc that is recoverable can be repositioned; a joint already destroyed beyond repair points toward total joint replacement instead.
Conservative care is weighed first. Many symptomatic joints improve with non-surgical management. Repositioning is reserved for displacement that is painful, progressive, or part of a planned skeletal correction.
The disc is secured, not just nudged. Returning the disc to position only helps if it stays — which is why it is anchored to bone rather than left to drift forward again.

The joint is stabilized before the jaws are moved. When facial asymmetry or a malocclusion is also being corrected, stabilizing the disc first gives the reconstruction a sound foundation, often within a single operation.
Success is defined honestly. Realistic goals are pain relief, restored and stable joint function, and protection of the joint over time — not a guarantee of a silent, perfect joint. Every surgery carries risk, and a candid discussion of those risks is part of informed consent.
Where This Care Happens
Dr. Wolford’s practice is located on the campus of Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 — minutes from downtown Dallas and accessible from across the Dallas–Fort Worth metroplex. Valet parking is available, with self-parking in the adjacent building.
Patients travel to Dallas from across the country and internationally for evaluation of complex joint problems. All procedures for both current and new patients are performed exclusively at the Dallas office. Out-of-town patients can review what to bring — including prior imaging and records — on the patient information page.
Frequently Asked Questions
What does it mean that my disc is displaced?
The articular disc is a cushion that should sit between the condyle and the skull base and move smoothly with the jaw. When it slips forward, the joint can click as the disc snaps in and out, or lock when the disc blocks movement. Left displaced over time, it can accelerate joint wear.
What is the Mitek anchor technique?
A method of returning the displaced disc to its correct position and securing it there with a small bone anchor and sutures, so the disc stays stabilized over the condyle rather than slipping forward again. Stabilizing the disc is intended to protect the joint surfaces.
Why not just live with the clicking?
Clicking alone is common and does not always need surgery. The concern is progression — pain, locking, limited opening, and joint breakdown. When displacement is symptomatic or part of a larger reconstructive plan, repositioning aims to stop that progression.
Is disc repositioning done alone or with other surgery?
Both. It may be done on its own for an unstable, symptomatic joint, or combined with corrective jaw surgery when a misaligned bite or facial asymmetry is also being treated.
Will repositioning the disc fix my bite?
Disc repositioning addresses the joint, not the alignment of the jaws. When the bite is also off, corrective jaw surgery is planned alongside it. Goals are pain relief, stable function, and protection of the joint — outcomes vary and are not guaranteed.
Related Reading on This Site
Authoritative Resources (External)
These independent, non-commercial sources offer further patient education:
- National Institute of Dental and Craniofacial Research (NIH) — temporomandibular disorders overview
- MSD Manual (professional reference) — internal derangement and TMJ disorders
- MedlinePlus (U.S. National Library of Medicine) — patient-friendly TMJ overview
A note on patient stories: Any patient example used in marketing for this practice should be either fully de-identified or used only with written patient authorization, consistent with HIPAA. Because this condition can affect minors, particular care should be taken with consent and de-identification. The scenarios described in this article are general and composite, not specific patients. This article is educational and is not a substitute for individualized medical advice.