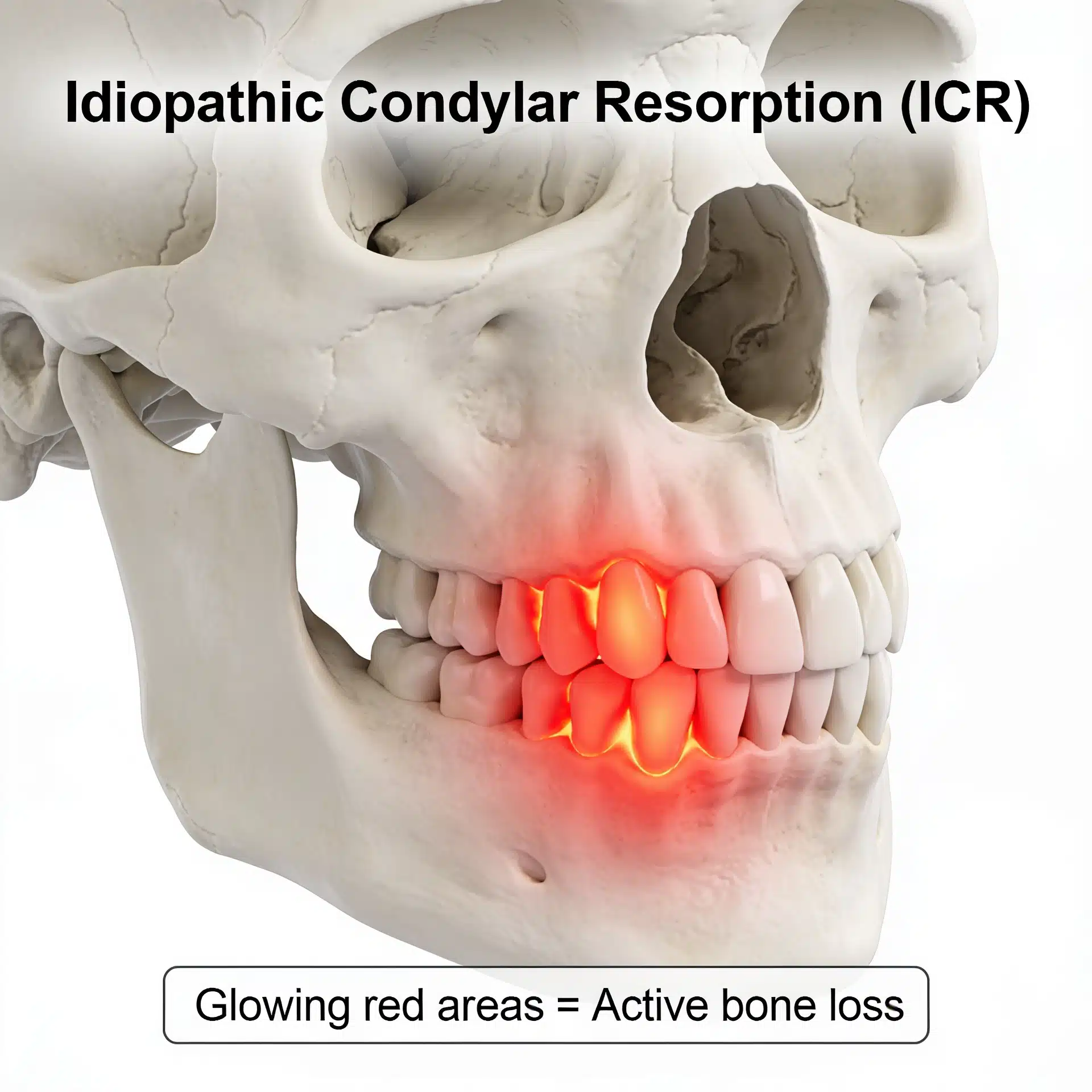
Idiopathic Condylar Resorption: When the Jaw Joint Quietly Dissolves
It usually starts as a bite that won’t behave. The front teeth stop meeting. The chin seems to be sliding backward in every new photo. An orthodontist closes the open bite, and within a year it reopens. There may be no joint pain at all — just a profile that keeps receding and a sense that the foundation underneath the teeth is shifting.
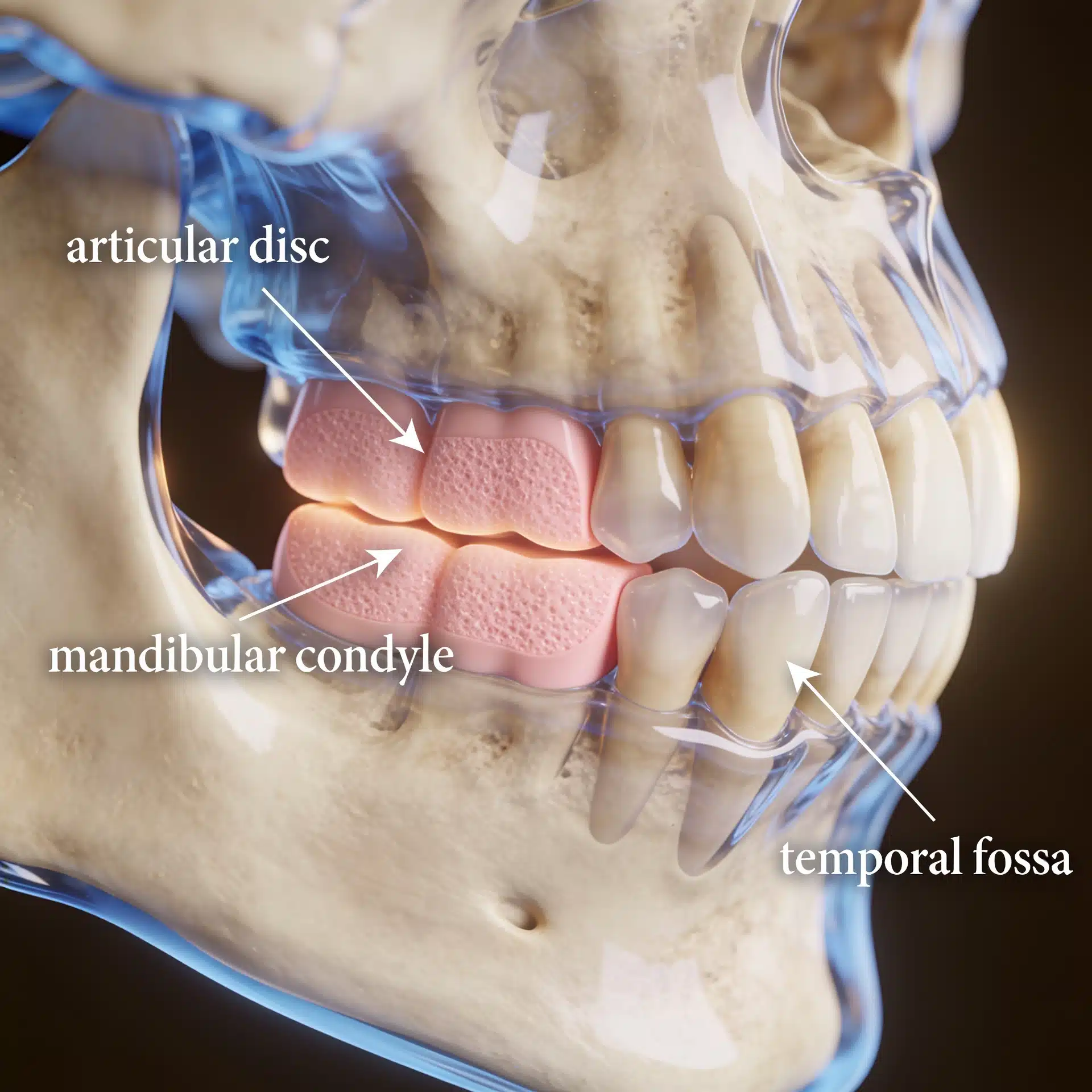
That shifting foundation is the point. In idiopathic condylar resorption (ICR), the condyles — the rounded tops of the lower jaw that form the jaw joints — slowly lose bone. As they shorten, the lower jaw rotates back and the bite opens. The teeth are not the problem; they are the readout of a joint that is breaking down. The first job is to find out whether that breakdown is still happening.
The Real Problem: A Jaw Joint Losing Its Own Bone
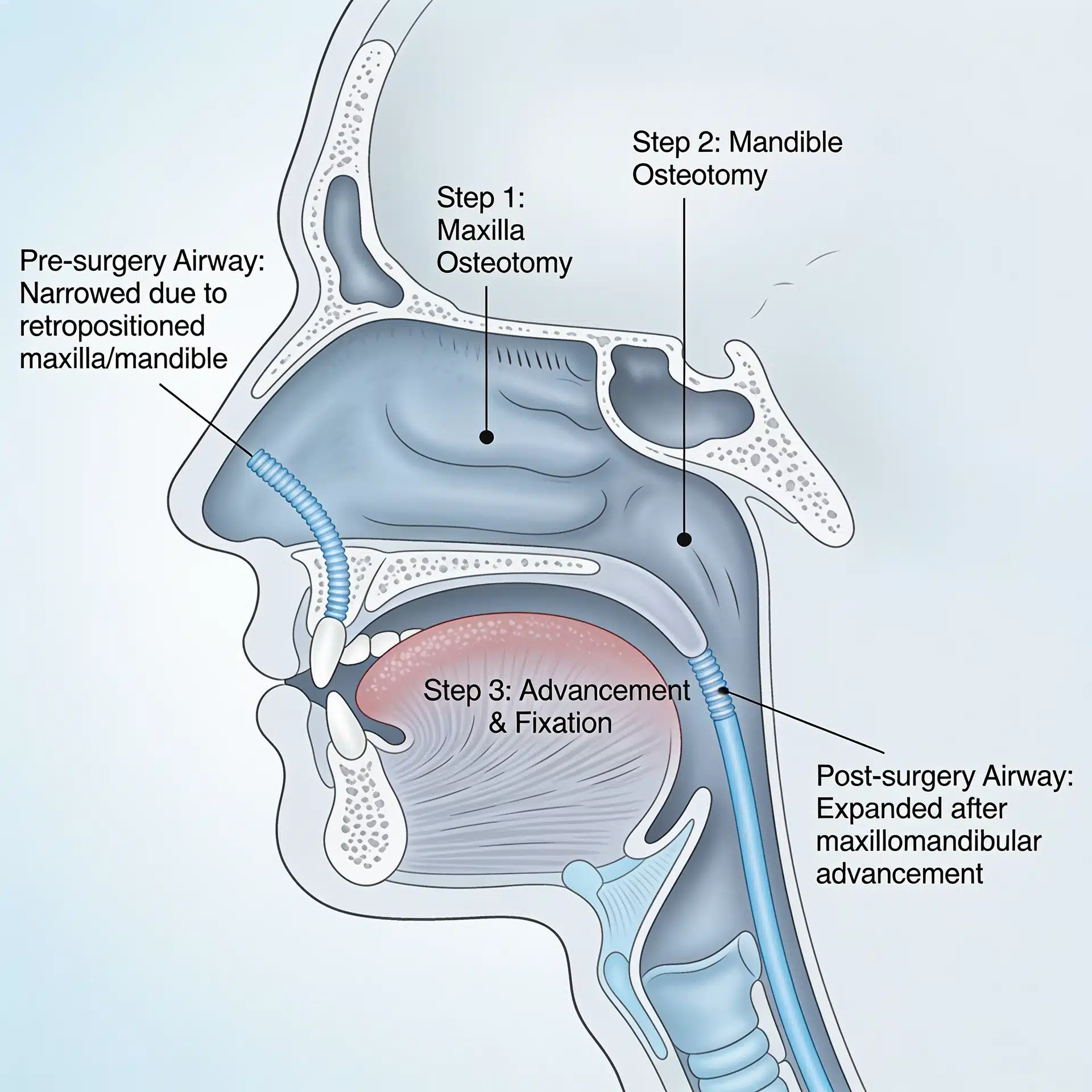
The condyle is both a hinge and a growth-and-remodeling center. In ICR, that remodeling tips toward destruction: the condylar head gradually resorbs, often on both sides, most commonly in adolescent and young-adult women. As condylar height is lost, the mandible swings backward and downward, producing a retruding chin, an anterior open bite and Class II malocclusion, and — because the lower jaw also crowds the airway as it retreats — sometimes new snoring or disrupted sleep.

ICR is easy to misread as ordinary orthodontics. A worsening open bite gets treated as a tooth problem while the engine driving it — a resorbing joint — keeps running. It sits at the opposite end of the same spectrum as condylar hyperplasia: one joint grows too much, the other dissolves. And although the cause is often called “idiopathic,” resorption can also be set off by prior jaw surgery, trauma, or an underlying connective-tissue or autoimmune disease, which is why a careful workup looks beyond the joint itself.

What an Experienced Surgeon Brings to the Decision
The hard part is not naming ICR — it is determining whether the resorption is active or burned out, and identifying anything feeding it, before committing to a plan. Operating on an actively resorbing joint without addressing the resorption predictably relapses.
Dr. Larry Wolford has more than four decades of experience treating jaw-joint disease and helped define how ICR is recognized and managed, including disc-repositioning approaches intended to stabilize the joint in selected active cases. When the joint can be salvaged, he repositions and secures the displaced disc; when it cannot, he performs reconstruction with a patient-fitted total joint prosthesis, frequently combined with corrective jaw surgery in one coordinated operation. That experience doesn’t change your anatomy, but it changes how accurately the cause is read and how completely it’s addressed.
Key Takeaways
- Idiopathic condylar resorption is progressive loss of condylar bone — a jaw-joint problem, not a simple bite problem.
- It causes a retruding chin, an opening bite, and sometimes airway changes, most often in adolescent and young-adult women, and is frequently painless.
- It is the mirror image of condylar hyperplasia: too little condyle rather than too much.
- Whether the resorption is still active is the decisive question — it dictates whether the joint can be salvaged or must be reconstructed.
- Correcting the bite while the joint is still resorbing tends to relapse. The joint process has to be stopped, not just the malocclusion masked.
- Goals are realistic: halt the resorption, restore facial balance and a functional bite, and protect the airway. Outcomes vary and are never guaranteed.
How the Decision Is Actually Made
Here is the reasoning behind that answer.
Diagnosis combines serial records and joint imaging. Comparing models, photos, and radiographs over time shows whether the bite and chin position are still changing. Cone-beam CT maps the bony loss, and an MRI evaluation of the TMJ shows the condition and position of the disc. The point is to separate disease that is still moving from disease that has stabilized.
Underlying drivers are ruled in or out. Because hormonal and autoimmune factors and prior surgery can all fuel resorption, evaluation looks for a treatable contributor rather than assuming the joint is acting alone.
The joint is salvaged when it still can be. In selected active cases, repositioning the displaced articular disc and anchoring it (Mitek anchor technique) is intended to halt the resorption and preserve the patient’s own joint — see articular disc repositioning.
The joint is reconstructed when it cannot be saved. When the condyle is severely resorbed or the disease is advanced, a custom total joint prosthesis rebuilds the joint and supports the lower face, commonly combined with repositioning of the jaws in a single stage. The related condition of overgrowth is covered under condylar hyperplasia.
Success is defined honestly. Realistic objectives are to stop the resorption, restore symmetry and a functional bite, and protect function and airway — not a guarantee of perfect or permanent symmetry. Every surgery carries risk, and a candid discussion of those risks is part of informed consent.
Where This Care Happens
Dr. Wolford’s practice is located on the campus of Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 — minutes from downtown Dallas and accessible from across the Dallas–Fort Worth metroplex. Valet parking is available, with self-parking in the adjacent building.
Because ICR is uncommon and frequently mistaken for ordinary malocclusion, patients and families travel to Dallas from across the country and internationally for evaluation. All procedures for both current and new patients are performed exclusively at the Dallas office. Out-of-town patients can review what to bring — including prior orthodontic records, imaging, and photos over time — on the patient information page.
Frequently Asked Questions
Why is my chin moving backward and my front teeth no longer touching?
As the condyles lose height, the lower jaw rotates back and down. That pulls the chin back and opens a gap between the front teeth. A progressive, often painless open bite in a teenager or young adult is a classic clue for ICR.
Does idiopathic condylar resorption hurt?
Sometimes there is joint pain, clicking, or limited opening — but many patients feel little or nothing. The bite change and receding chin are often the first signs, and absence of pain does not mean the resorption has stopped.
How do you know whether the resorption is still active?
By comparing records over time and reviewing joint imaging. Serial photos, models, and radiographs show whether the bite and chin are still changing, while MRI and other imaging assess the joint and disc. Active and burned-out disease are treated differently.
Can braces fix it?
Orthodontics can move teeth but cannot rebuild a resorbing condyle or stop the process. Used alone on active disease, the correction tends to relapse. The joint problem has to be addressed.
Will I need a jaw-joint replacement?
Not always. In selected active cases, repositioning and stabilizing the disc may halt the process and preserve the joint. When the condyle is severely destroyed, a patient-fitted total joint replacement may be more predictable. Candidacy is individual.
Related Reading on This Site
Authoritative Resources (External)
These independent, non-commercial sources offer further patient education:
- National Institute of Dental and Craniofacial Research (NIH) — temporomandibular disorders overview for general jaw-joint context
- MSD Manual (professional reference) — temporomandibular disorders, including condylar conditions
- National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIH) — background on joint and bone disorders
A note on patient stories: Any patient example used in marketing for this practice should be either fully de-identified or used only with written patient authorization, consistent with HIPAA. Because this condition often affects minors, particular care should be taken with consent and de-identification. The scenarios described in this article are general and composite, not specific patients. This article is educational and is not a substitute for individualized medical advice.