Total TMJ Replacement: Rebuilding a Joint That Can No Longer Be Saved
By the time most people reach this conversation, they have been through a lot. The jaw locks halfway open, or barely opens at all. Chewing is a negotiation. There may have been one surgery already — sometimes several — and an old implant that failed and left things worse. The question is no longer how to calm an irritated joint. The joint is gone. The question is how to replace it.
A total temporomandibular joint replacement does exactly that: it removes a destroyed joint and rebuilds it with an artificial one. It is not a treatment for everyday clicking or routine jaw pain. It is reconstructive surgery for an end-stage joint — and deciding that a joint has truly reached that point is the most important judgment in the whole process.
The Real Problem: An End-Stage Joint
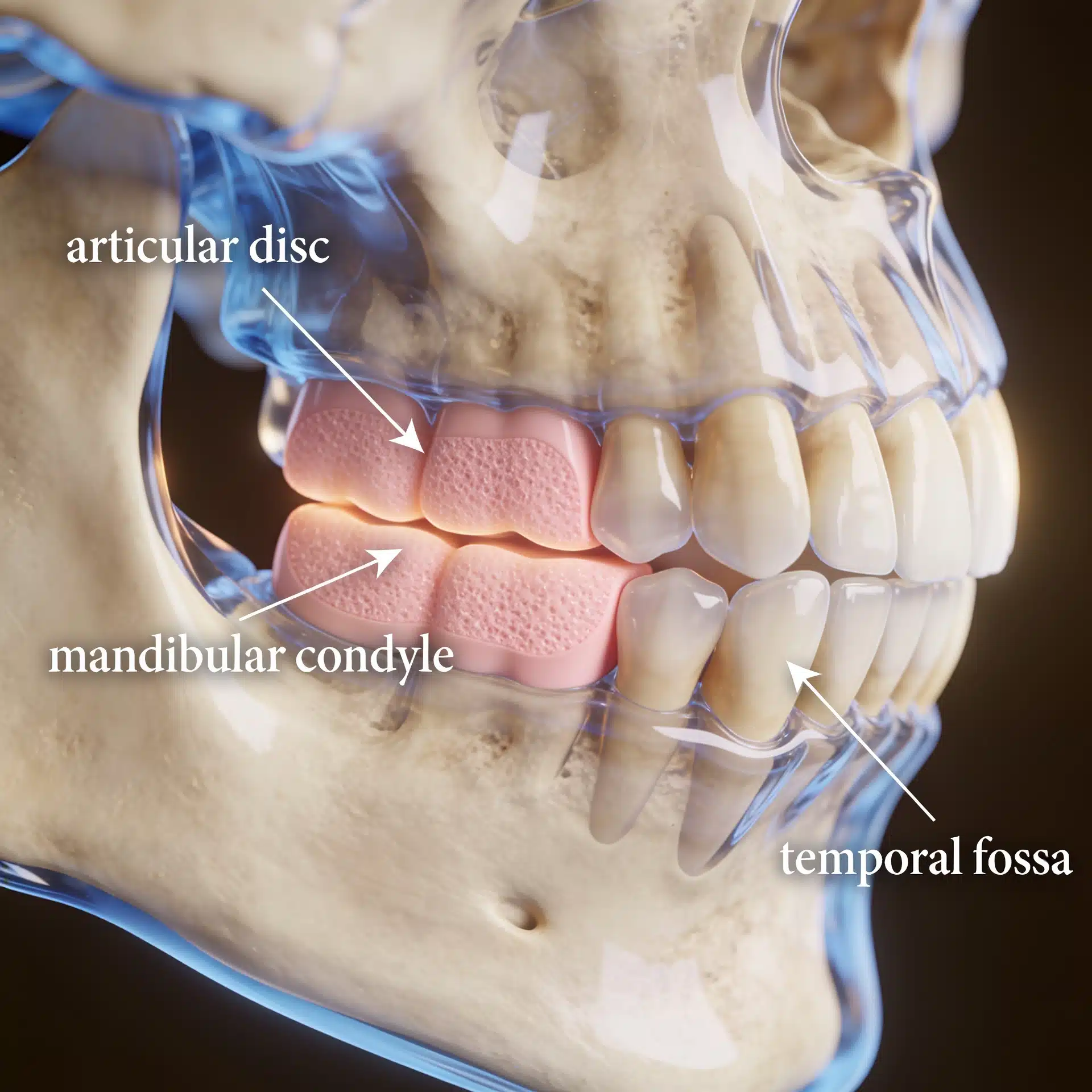
The TMJ is a small joint doing a large job, and a handful of conditions can destroy it beyond repair. Severe degenerative arthritis wears the joint surfaces away. Advanced idiopathic condylar resorption dissolves the condyle. Ankylosis fuses the joint to the skull base so the mouth can barely open. Tumors, trauma, certain autoimmune and connective-tissue diseases, congenital absence of the joint, and failed previous TMJ surgery — including older implants now known to have broken down — all land in the same place: a joint that no amount of conservative care or disc surgery can restore.
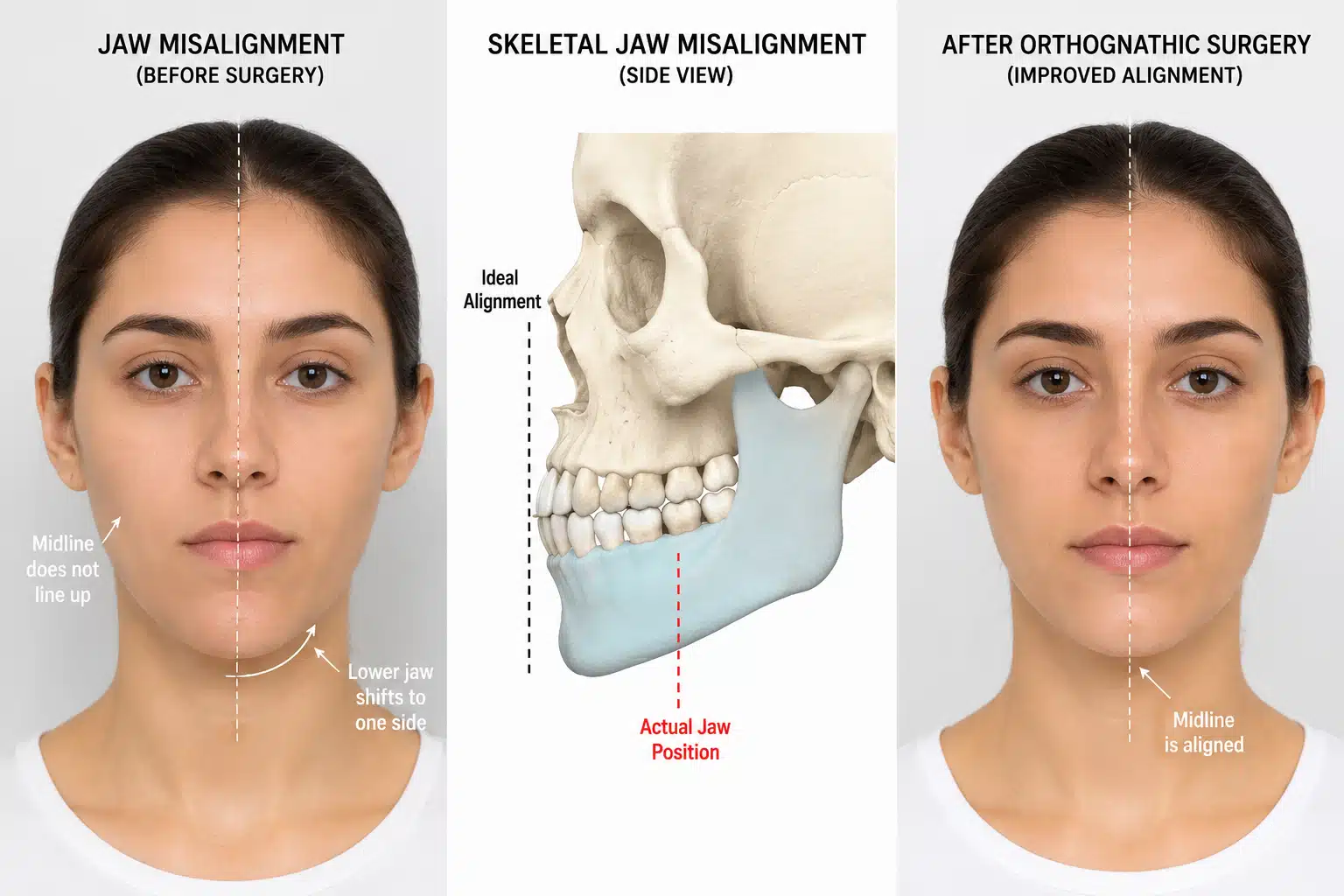
When the joint is that far gone, the lower jaw has usually shifted with it — a receding chin, a canted or open bite, a crowded airway. So the problem is rarely just the joint in isolation; it is the joint and the face and the bite together. That is what a well-planned reconstruction has to address.

What an Experienced Surgeon Brings to the Decision
The value of a focused practice here is twofold: knowing when a joint can still be salvaged with the patient’s own tissue versus when it genuinely needs replacement, and then planning the replacement so it corrects the face and bite — not only the joint.
Dr. Larry Wolford has spent more than four decades reconstructing damaged jaw joints and is widely published on total joint replacement and the technique of combining it with corrective jaw surgery. Many of his patients are people whose earlier operations elsewhere did not hold; reconstruction in a multiply-operated joint is its own discipline. He uses patient-fitted prostheses designed from each patient’s own CT anatomy, frequently performing the joint replacement and the jaw repositioning in one coordinated operation. That experience doesn’t change your anatomy — but it changes how completely the joint, the bite, and the airway are corrected.
Key Takeaways
- Total TMJ replacement is reconstruction for an end-stage joint, not a treatment for ordinary jaw pain or clicking.
- It is considered for severe arthritis, advanced resorption, ankylosis, tumors, certain autoimmune diseases, congenital absence, and failed prior surgery or implants.
- A patient-fitted prosthesis is built from your own CT anatomy, so it can also reposition the jaw and support the airway.
- Joint replacement is frequently combined with corrective jaw surgery in a single operation to rebalance the face and bite.
- Goals are to relieve pain, restore stable function, and stop joint destruction — not to recreate a perfect natural joint.
- Outcomes vary and are never guaranteed; recovery includes physical therapy and long-term follow-up.
How the Decision Is Actually Made
Here is the reasoning behind that answer.
Salvage is ruled out first. Before replacing a joint, the question is whether it can still be saved — for example by repositioning the articular disc. Replacement is reserved for joints where that option is gone.
Imaging drives the design. Cone-beam CT maps the bone for the custom device, and an MRI evaluation of the TMJ characterizes the soft tissue and disc. A patient-fitted prosthesis is then manufactured to the individual’s anatomy.

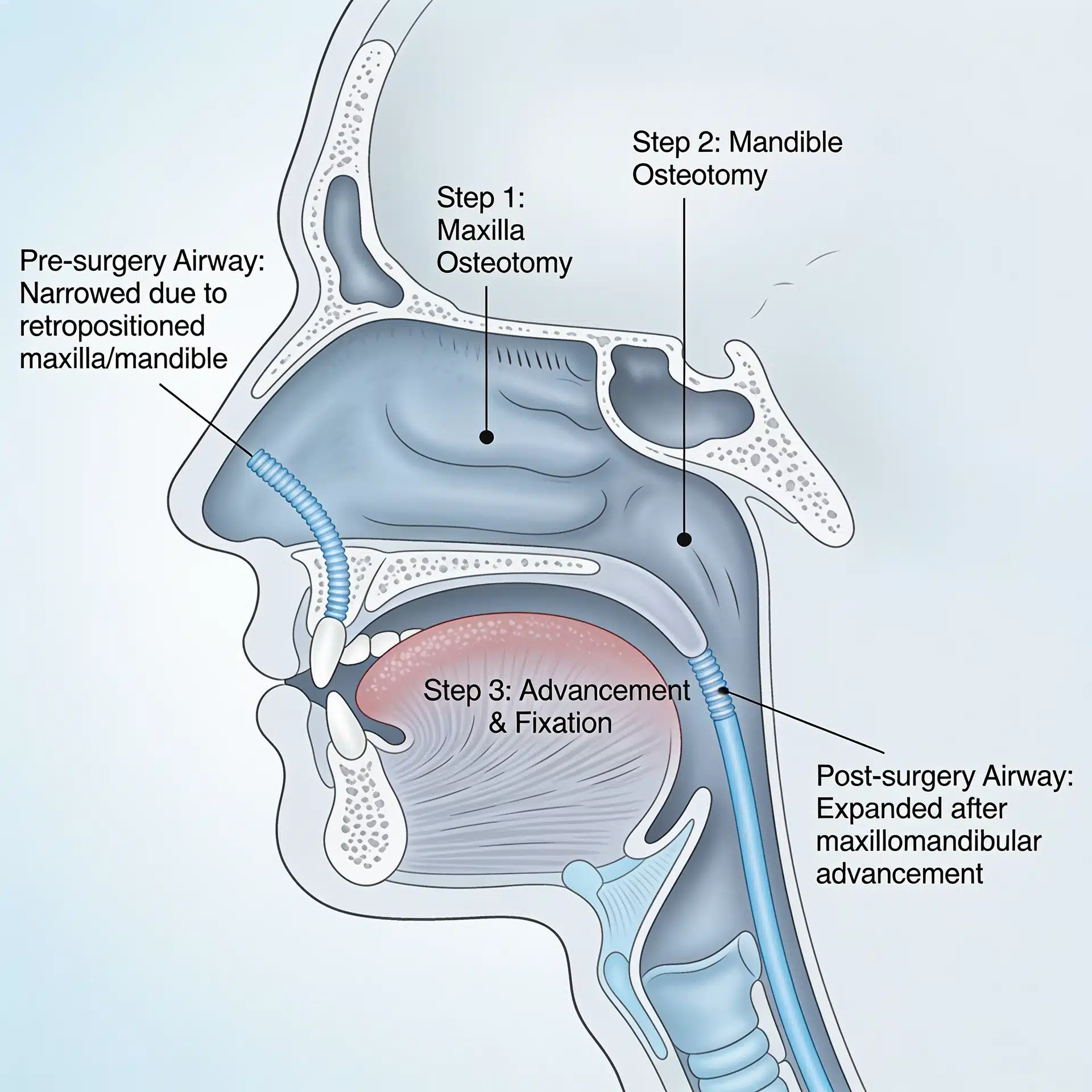
The face and bite are corrected at the same time. Because an end-stage joint usually drags the bite and profile with it, the prosthesis is planned together with orthognathic surgery so the jaws can be repositioned and the airway supported in one operation.
Recovery is planned, not improvised. Physical therapy to maintain opening, a managed diet progression, and long-term follow-up are built into the plan from the start.
Success is defined honestly. Realistic objectives are pain relief, stable function, a working bite, and an end to ongoing destruction — not a guarantee of a normal joint or perfect symmetry. Every surgery carries risk, and a candid discussion of those risks is part of informed consent.
Where This Care Happens
Dr. Wolford’s practice is located on the campus of Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 — minutes from downtown Dallas and accessible from across the Dallas–Fort Worth metroplex. Valet parking is available, with self-parking in the adjacent building.
Patients and families travel to Dallas from across the country and internationally for joint reconstruction, often after care elsewhere did not resolve the problem. All procedures for both current and new patients are performed exclusively at the Dallas office. Out-of-town patients can review what to bring — including prior surgical and imaging records — on the patient information page.
Frequently Asked Questions
Who actually needs a total TMJ replacement?
It is generally reserved for end-stage joints: severe arthritis, advanced condylar resorption, bony ankylosis, tumors involving the joint, failed prior TMJ surgery or older implants, and severe congenital absence of the joint. It is not a first step for ordinary jaw pain or clicking.
What is a patient-fitted (custom) prosthesis?
A two-part joint — a metal condyle and a fossa component — manufactured from a CT-based 3D model of your own anatomy so it matches your bone precisely. Because it is built to the individual, it can be designed to reposition the jaw and support the airway at the same time.
Can the jaw be straightened during the same operation?
Often yes. In many cases the joint replacement and corrective jaw surgery are planned together so the jaws can be repositioned, the bite leveled, and the lower face and airway improved in a single coordinated procedure.
Will I be able to open and chew normally afterward?
The goals are to relieve pain, restore stable function and a working bite, and stop further destruction. Many patients regain comfortable function, though opening may be more limited than a healthy natural joint, and physical therapy is part of recovery. Outcomes vary and are never guaranteed.
How long does a TMJ prosthesis last?
Modern total joint prostheses are designed for long-term function, and many remain in service for many years. Longevity depends on the individual, the underlying disease, and how the device is loaded; long-term follow-up is part of the plan.
Related Reading on This Site
Authoritative Resources (External)
These independent, non-commercial sources offer further patient education:
- National Institute of Dental and Craniofacial Research (NIH) — temporomandibular disorders overview
- American Association of Oral and Maxillofacial Surgeons — professional society patient resources
- U.S. Food and Drug Administration — information on temporomandibular joint implants
A note on patient stories: Any patient example used in marketing for this practice should be either fully de-identified or used only with written patient authorization, consistent with HIPAA. Because this condition can affect minors, particular care should be taken with consent and de-identification. The scenarios described in this article are general and composite, not specific patients. This article is educational and is not a substitute for individualized medical advice.