When an Autoimmune Disease Attacks the Jaw Joint
The diagnosis is already on the chart — rheumatoid arthritis, lupus, juvenile arthritis, something with a long name and a longer medication list. What no one warned about was the jaw. The bite that slowly stopped meeting in front. The chin sliding backward. The morning stiffness that now includes the jaw joint, the opening that keeps shrinking. The disease that has been working on the hands and knees has found the temporomandibular joint too.
That is the heart of it: the TMJ is a joint like any other, and the diseases that attack joints can attack it. Treating the joint without treating the disease behind it is like bailing a boat without finding the leak. These cases call for two kinds of care at once.
The Real Problem: A Joint Caught in a Systemic Disease
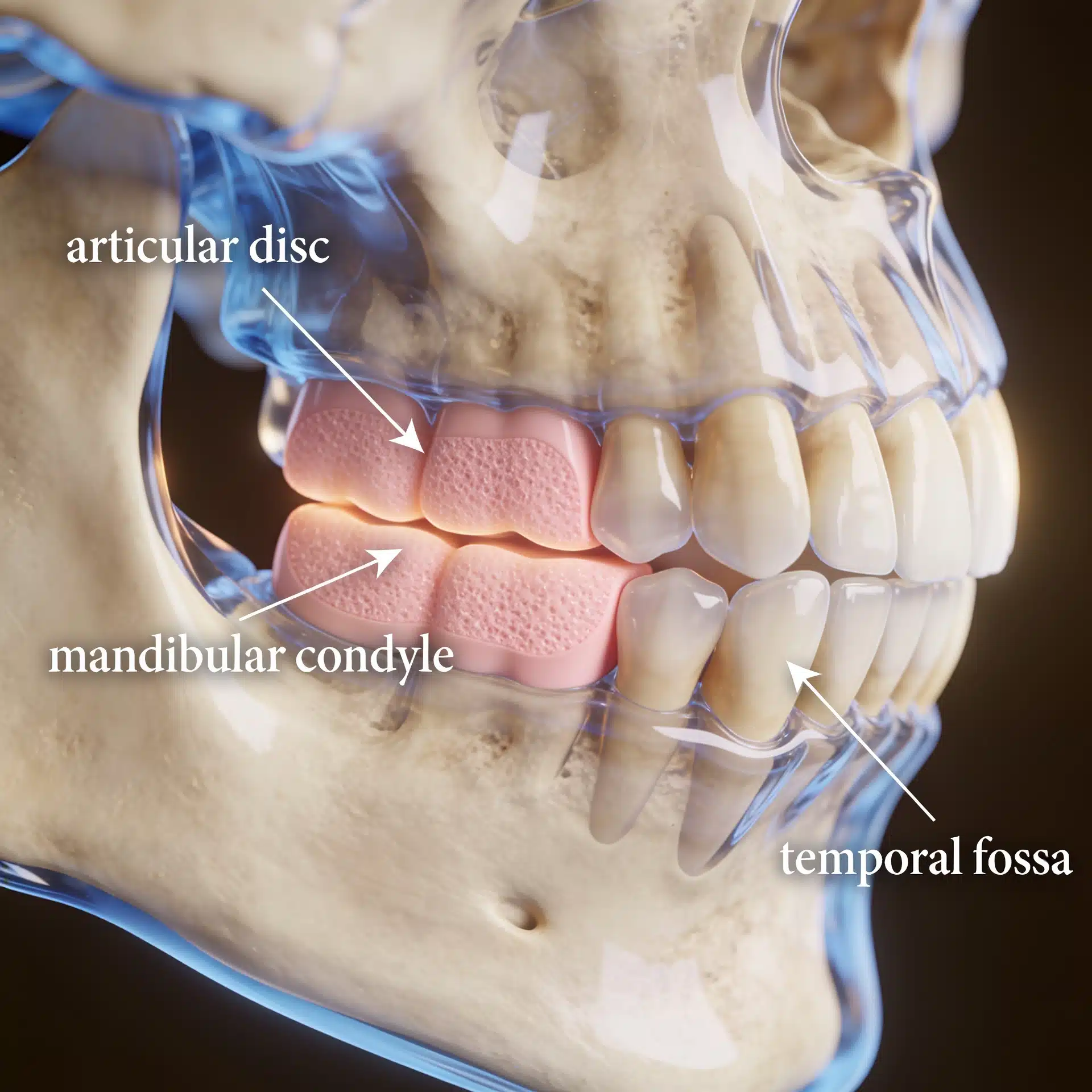
The temporomandibular joint is a synovial joint — the same kind of lined, fluid-filled joint as the knee or knuckle. That makes it a target for the inflammatory and connective-tissue diseases that target joints elsewhere: rheumatoid arthritis, juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis, lupus, scleroderma, and reactive arthritis among them. The inflammation erodes the joint surfaces and can dissolve the condyle outright.
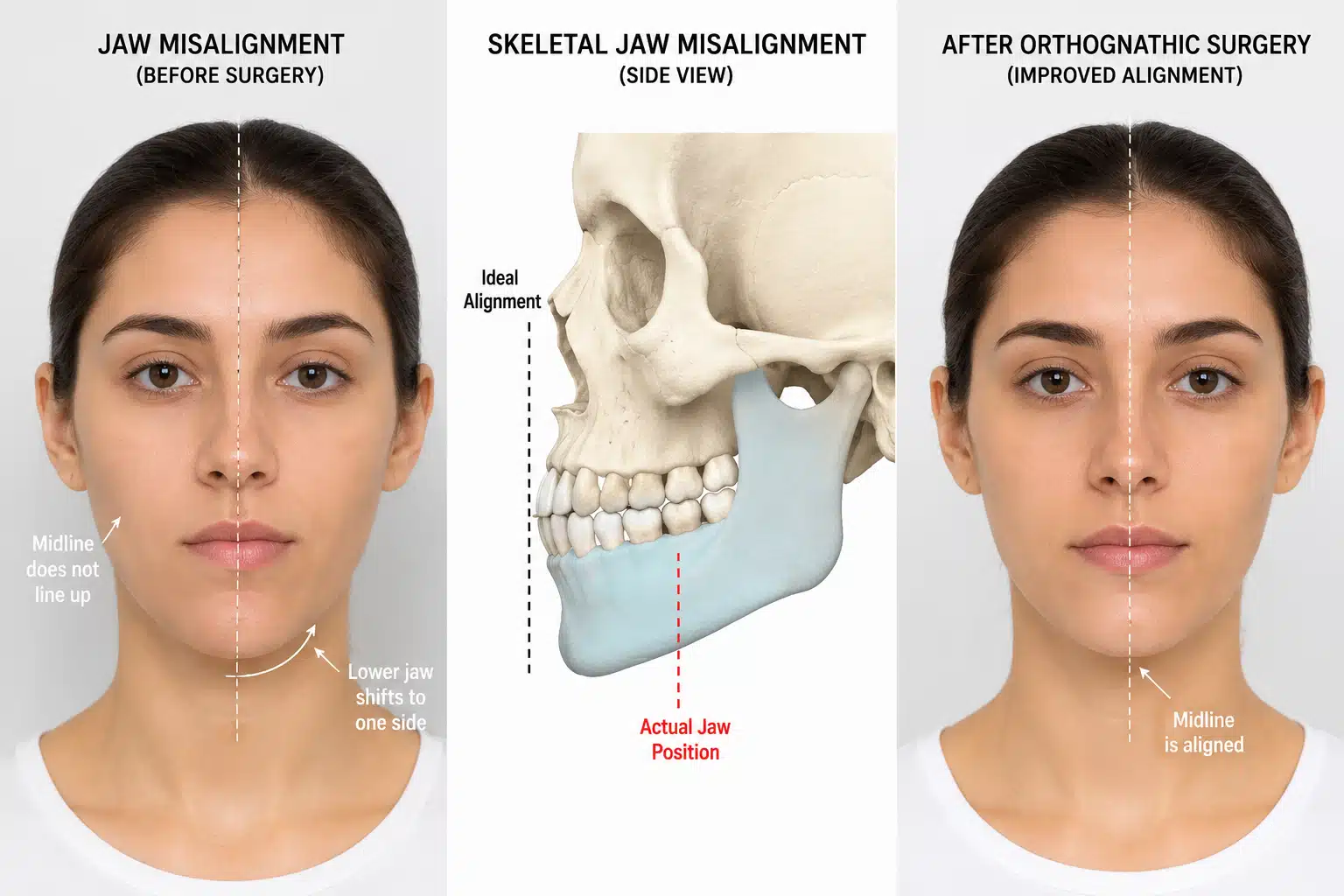
As the condyle is destroyed, the consequences mirror condylar resorption: the jaw rotates backward, the chin recedes, and an anterior open bite develops, often with pain and shrinking opening. In children with juvenile arthritis, joint involvement can disturb jaw growth and produce facial asymmetry and underdevelopment. The bite and the face are the visible signs; the engine is a systemic disease, and that is what makes these among the most demanding TMJ problems to manage.

What an Experienced Surgeon Brings to the Decision
The decisive judgments are recognizing that a systemic disease — not a local joint problem — is driving the damage, coordinating with the physicians controlling that disease, and timing any surgery so it isn’t undone by ongoing inflammation.
Dr. Larry Wolford has more than four decades of experience treating jaw joints affected by connective-tissue and autoimmune disease and has published on their surgical management, including reconstruction of joints damaged by inflammatory disease. He works alongside the patient’s rheumatologist or physician so the disease is controlled medically while the joint, bite, and face are addressed surgically. That experience doesn’t change your anatomy or your underlying diagnosis, but it changes how clearly the cause is recognized and how completely the joint and face are restored once the disease is under control.
Key Takeaways
- The TMJ is a synovial joint, so autoimmune and connective-tissue diseases that attack joints can damage it too.
- Conditions involved include rheumatoid arthritis, juvenile idiopathic arthritis, lupus, psoriatic arthritis, ankylosing spondylitis, scleroderma, and reactive arthritis.
- Inflammation can erode and dissolve the condyle, producing pain, a progressive open bite, a receding chin, and facial asymmetry.
- In children, joint involvement can disturb jaw growth and facial development.
- Surgery alone isn’t enough — the systemic disease must be controlled medically, in coordination with the treating physician.
- Treatment ranges from joint-preserving surgery to total joint replacement with corrective jaw surgery; outcomes vary and are never guaranteed.
How the Decision Is Actually Made
Here is the reasoning behind that answer.
The systemic cause is identified. Because the bite and joint changes can look like a purely local problem, recognizing the underlying disease — sometimes with input from a rheumatologist — is the first and most important step.
Imaging defines the joint damage. Cone-beam CT shows how much condylar bone has been lost, and an MRI evaluation of the TMJ assesses inflammation and the disc, separating salvageable joints from destroyed ones.

The disease is controlled before the joint is rebuilt. Operating into active, uncontrolled inflammation risks losing the result, so surgical timing and medication are planned with the treating physician.
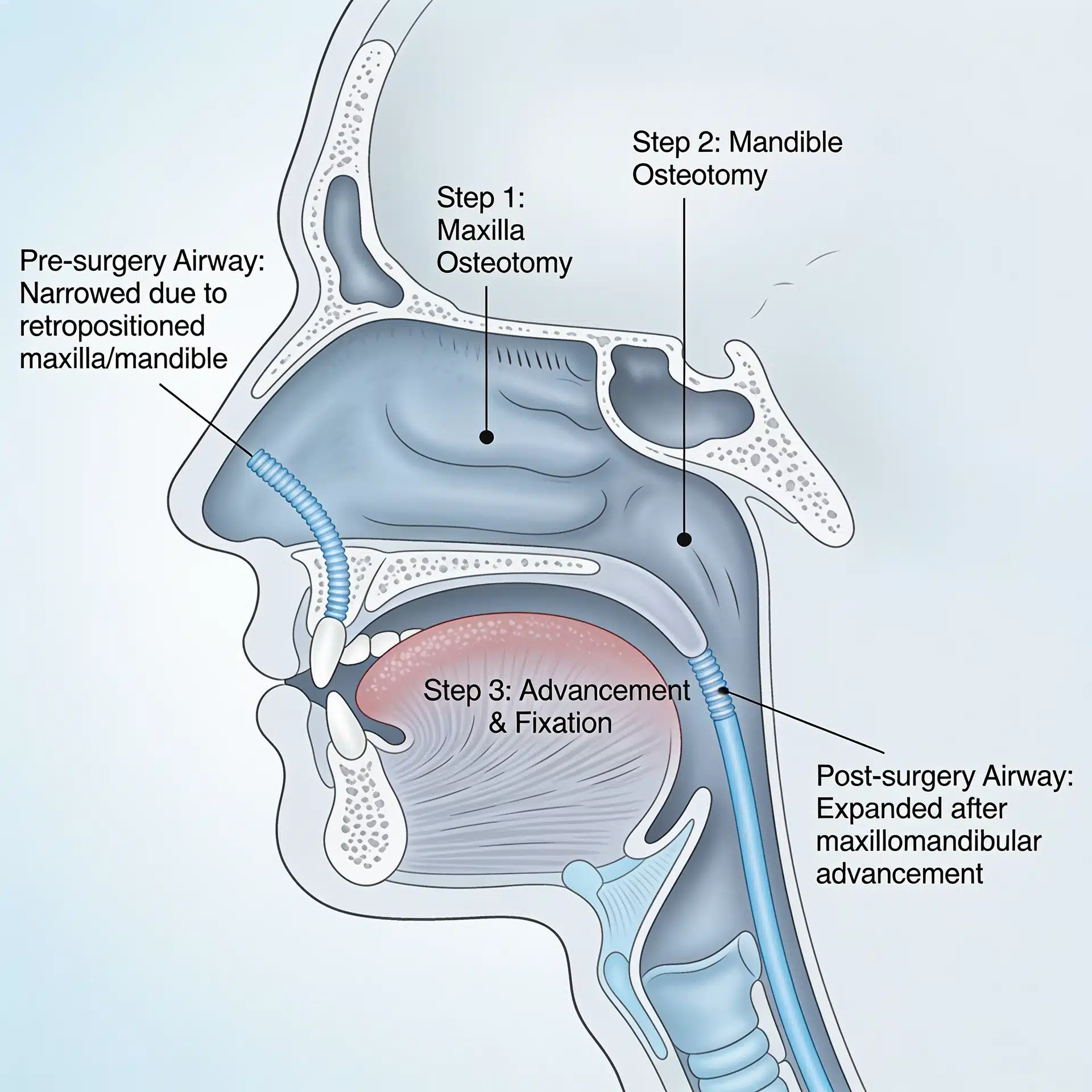
The joint is preserved or reconstructed accordingly. Less-damaged joints may respond to disc repositioning and joint-preserving surgery; severely destroyed joints may need a total joint replacement, frequently with jaw repositioning to rebalance the bite and face.
Success is defined honestly. Realistic goals are to relieve pain, restore function and a working bite, and stabilize the joint while the disease is managed elsewhere — not a cure for the underlying autoimmune condition or a guarantee of perfect symmetry. Every surgery carries risk, and a candid discussion of those risks is part of informed consent.
Where This Care Happens
Dr. Wolford’s practice is located on the campus of Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 — minutes from downtown Dallas and accessible from across the Dallas–Fort Worth metroplex. Valet parking is available, with self-parking in the adjacent building.
Patients with autoimmune joint disease travel to Dallas from across the country and internationally, often because the jaw involvement is uncommon and easily overlooked. All procedures for both current and new patients are performed exclusively at the Dallas office. Out-of-town patients can review what to bring — including rheumatology records, medication lists, and prior imaging — on the patient information page.
Frequently Asked Questions
Can a disease like rheumatoid arthritis really affect the jaw joint?
Yes. The temporomandibular joint is a synovial joint like the knee or hand, so conditions such as rheumatoid arthritis, juvenile idiopathic arthritis, lupus, psoriatic arthritis, and ankylosing spondylitis can inflame and damage it — sometimes destroying the condyle and changing the bite and face.
Why does my bite keep changing if it’s an autoimmune disease?
As inflammation erodes the condyles, they lose height, the lower jaw rotates back, and the front teeth stop meeting — a progressive open bite and receding chin. The bite change is a downstream sign that the joint is being destroyed.
Do I need to see a rheumatologist as well as a surgeon?
Usually, yes. When a systemic disease is driving the joint damage, controlling that disease medically is essential. Surgery on the joint without controlling the underlying disease risks ongoing destruction, so the two are coordinated.
Can the joint be repaired, or does it need replacement?
It depends on how much damage has occurred and whether the disease is controlled. Less-damaged joints may be managed with joint-preserving surgery; severely destroyed joints may need a patient-fitted total joint replacement, often with corrective jaw surgery. Candidacy is individual.
Is it safe to operate while I’m on immune-suppressing medication?
Timing and medication management are planned together with the treating physician, because some medications affect healing and infection risk. This coordination is part of why these cases are managed as a team. Outcomes vary and are never guaranteed.
Related Reading on This Site
Authoritative Resources (External)
These independent, non-commercial sources offer further patient education:
- National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIH) — rheumatoid arthritis and related disease overviews
- American College of Rheumatology — patient education on autoimmune and inflammatory joint disease
- National Institute of Dental and Craniofacial Research (NIH) — temporomandibular joint context
A note on patient stories: Any patient example used in marketing for this practice should be either fully de-identified or used only with written patient authorization, consistent with HIPAA. Because these conditions often affect minors (for example, juvenile idiopathic arthritis), particular care should be taken with consent and de-identification. The scenarios described in this article are general and composite, not specific patients. This article is educational and is not a substitute for individualized medical advice.