Maxillomandibular Advancement: Treating Sleep Apnea at the Airway Itself
The mask helped, at first. Then it didn’t stay on, or the straps left marks, or the noise kept a partner awake, or it simply ended up on the nightstand more nights than not. Meanwhile the daytime fog never quite lifted — the 3 p.m. crash, the microsleeps at the wheel, the blood pressure that won’t behave. For a subset of people with obstructive sleep apnea, the airway keeps collapsing not because the device is wrong, but because of where the jaws sit.
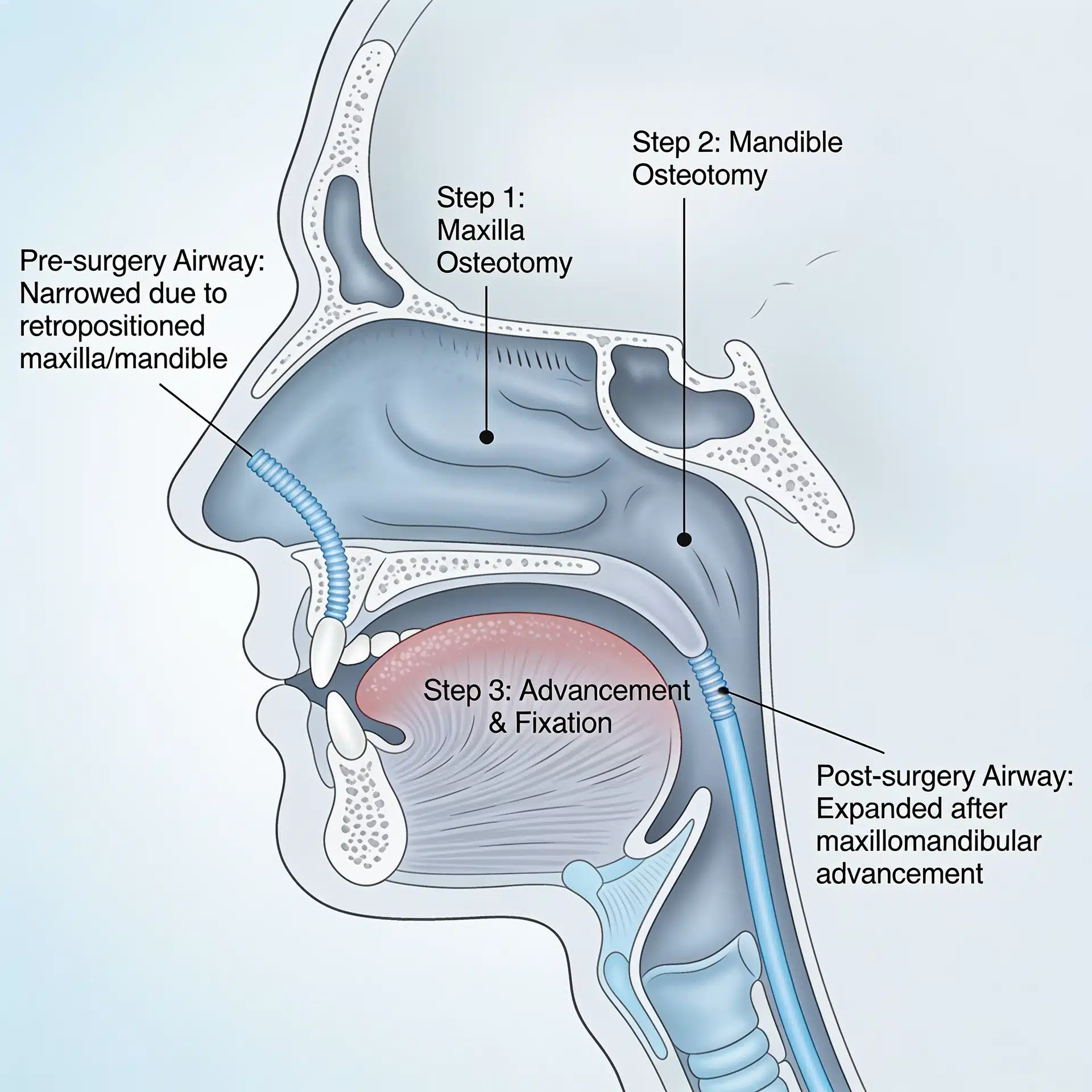
Maxillomandibular advancement (MMA) addresses that directly. Instead of holding the airway open from the outside every night, it enlarges the airway from within by moving both jaws forward. It is not a first move for everyone — but for the right patient, it treats the structure, not just the symptom.
The Real Problem: An Airway That Collapses During Sleep
In obstructive sleep apnea, the muscles relax during sleep and the soft tissues of the throat, tongue, and palate fall back and block the airway — over and over, all night. Each collapse drops oxygen and jolts the body awake just enough to breathe. The downstream toll is well known: relentless fatigue, impaired concentration, and links to high blood pressure, heart disease, and other serious conditions.
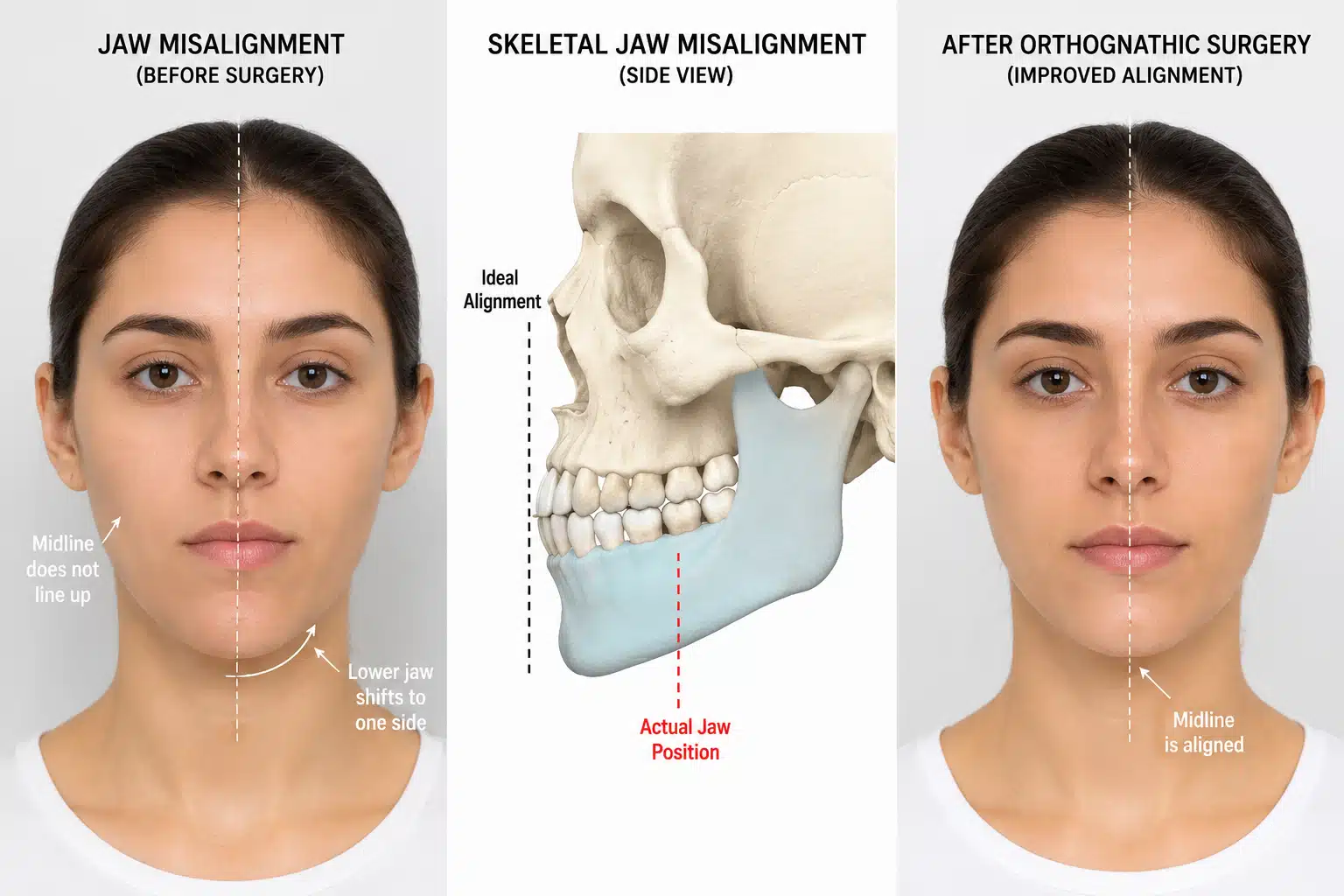
CPAP is the standard first-line therapy and works well when it is tolerated. But not everyone can use it consistently, and in some people the underlying problem is skeletal — jaws positioned in a way that leaves little room behind the tongue and palate. When the bony framework is part of the cause, addressing the jaws can address the airway. This is closely related to corrective jaw surgery for bite and facial balance, applied here with the airway as the goal.

What an Experienced Surgeon Brings to the Decision
The key judgments are whether the jaw structure is genuinely a major driver of the airway collapse, and how to plan the advancement so it enlarges the airway while keeping the bite and face in balance.
Dr. Larry Wolford has more than four decades of experience in orthognathic and airway surgery and has published widely on jaw repositioning, including techniques that rotate and advance the jaws to expand the airway. Because MMA is fundamentally corrective jaw surgery, he can plan the airway, the bite, and facial proportions together. This work is coordinated with the patient’s sleep physician, whose diagnosis and follow-up testing remain central. That experience doesn’t change your anatomy, but it changes how precisely the airway is planned and how well the bite and face are preserved.
Key Takeaways
- Obstructive sleep apnea is repeated airway collapse during sleep, with serious downstream health effects.
- CPAP is the standard first-line therapy; MMA is considered mainly when CPAP fails or isn’t tolerated, or when jaw structure is a major contributor.
- Maxillomandibular advancement moves both jaws forward, pulling the tongue and palate tissues with them and enlarging the airway.
- Because it is a form of corrective jaw surgery, the airway and the bite can be planned and corrected together.
- Diagnosis and follow-up rest with a sleep physician, including sleep studies before and after surgery.
- In well-selected patients it can markedly reduce apnea severity, but it is not guaranteed to eliminate apnea in everyone. Outcomes vary.
How the Decision Is Actually Made
Here is the reasoning behind that answer.
Diagnosis and severity come from sleep medicine. A sleep physician confirms obstructive sleep apnea and its severity with a sleep study; surgery is built on that foundation, not in place of it.
The airway is mapped. Imaging, including cone-beam CT, shows where the airway is narrow and how far the jaws can be advanced, so the surgical plan is specific to the individual’s anatomy.
The bite and face are planned with the airway. Because advancing the jaws changes occlusion and profile, the plan balances airway gain with a functional bite and facial harmony — the same principles used in orthognathic surgery.
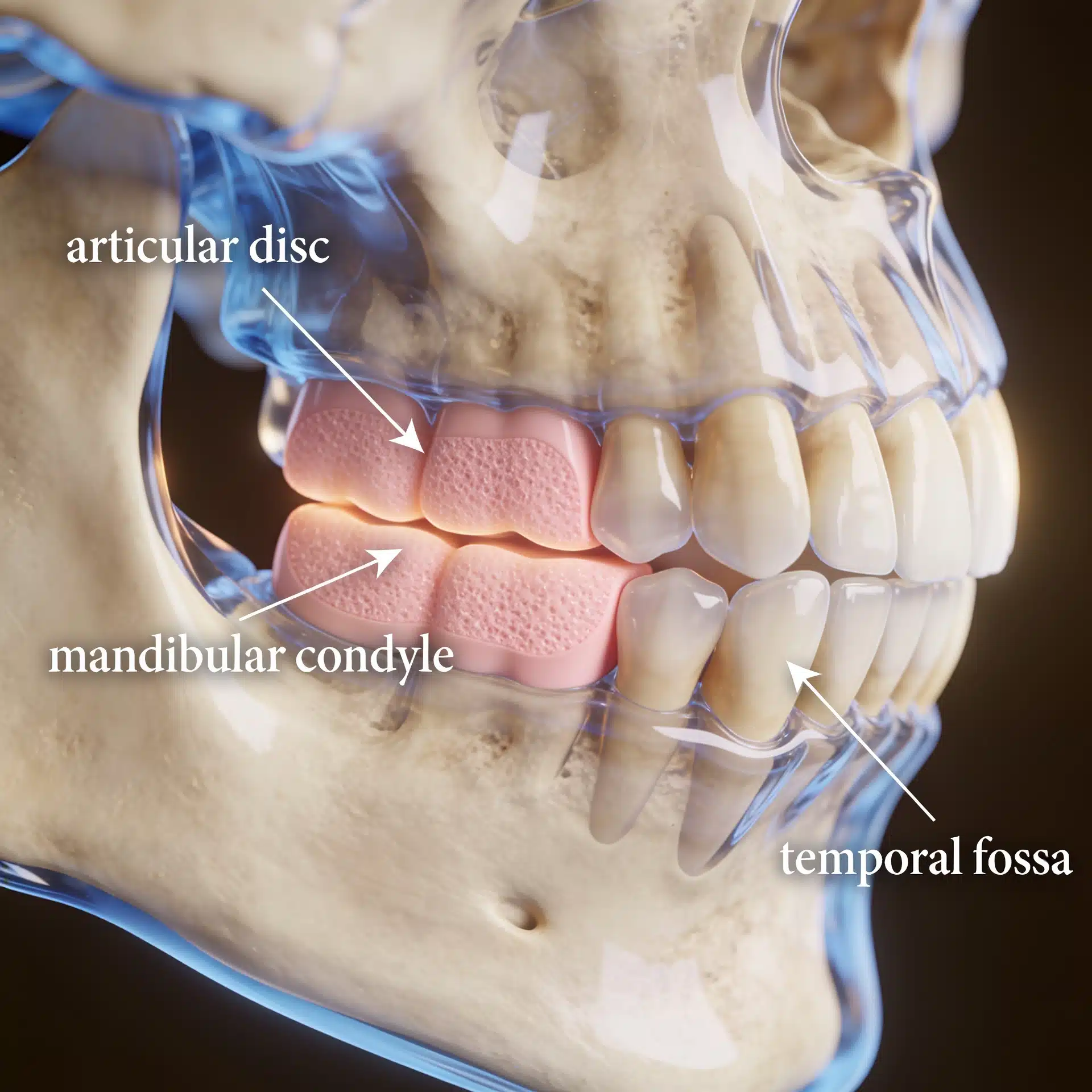
The joints are accounted for. Healthy temporomandibular joints make jaw advancement more stable; when joint disease is present, it is evaluated first — see MRI evaluation for TMJ and, where relevant, joint reconstruction.
Success is defined honestly. Realistic goals are a meaningful reduction in apnea severity, better sleep and daytime function, and a balanced bite and face — not a guaranteed cure for every patient. Follow-up sleep testing measures the result. Every surgery carries risk, and a candid discussion of those risks is part of informed consent.
Where This Care Happens
Dr. Wolford’s practice is located on the campus of Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 — minutes from downtown Dallas and accessible from across the Dallas–Fort Worth metroplex. Valet parking is available, with self-parking in the adjacent building.
Patients travel to Dallas from across the country and internationally for airway and jaw surgery. All procedures for both current and new patients are performed exclusively at the Dallas office. Out-of-town patients can review what to bring — including sleep studies and prior imaging — on the patient information page.
Frequently Asked Questions
How does moving my jaws forward help sleep apnea?
In obstructive sleep apnea the airway collapses during sleep. Advancing the upper and lower jaws pulls the attached tongue and palate tissues forward with them, enlarging the space behind them so the airway is less likely to collapse. It treats the airway at a skeletal level rather than with a nightly device.
Is this only for people who can’t tolerate CPAP?
It is most often considered when CPAP and other measures have failed or aren’t tolerated, or when the jaw structure itself is a major contributor to airway collapse. A sleep physician’s diagnosis with a sleep study, and a coordinated evaluation, guide whether surgery is appropriate.
Will surgery change how my face looks?
Advancing the jaws changes the lower-face profile, often supporting the chin and jawline. Surgical planning accounts for both airway and facial balance, and what to expect is discussed in detail beforehand.
Can it be combined with correcting my bite?
Yes. Maxillomandibular advancement is a form of corrective jaw surgery, so when the bite or facial proportions also need correction, the airway and the bite can be addressed together in the same plan.
Does it cure sleep apnea?
In well-selected patients, MMA can substantially reduce apnea severity, and many improve markedly. It is not guaranteed to eliminate apnea in every patient, and ongoing follow-up with a sleep physician, including a repeat sleep study, is part of care. Outcomes vary.
Related Reading on This Site
Authoritative Resources (External)
These independent, non-commercial sources offer further patient education:
- National Heart, Lung, and Blood Institute (NIH) — sleep apnea overview
- American Academy of Sleep Medicine (Sleep Education) — patient education on obstructive sleep apnea
- American Association of Oral and Maxillofacial Surgeons — corrective jaw and airway surgery resources
A note on patient stories: Any patient example used in marketing for this practice should be either fully de-identified or used only with written patient authorization, consistent with HIPAA. The scenarios described in this article are general and composite, not specific patients. Diagnosis and management of obstructive sleep apnea require evaluation by a qualified sleep physician; this article is educational and is not a substitute for individualized medical advice.