Medically reviewed and authored by Larry M. Wolford, DMD — Board-Certified Oral & Maxillofacial Surgeon, Dallas, TX. Last reviewed: May 2026.
Educational disclaimer: This article is for general educational purposes and is not a substitute for an individualized medical evaluation. Most jaw-joint symptoms are managed without surgery; whether any procedure is appropriate can only be determined through examination and imaging. No outcome is guaranteed; results vary by patient.
First it’s a click. The jaw pops when you yawn or take a big bite, maybe a little tender afterward, easy to ignore. Then the click starts catching — the jaw hesitates before it opens, like a drawer sticking on its track. And then, for some people, comes the morning it simply won’t open. The jaw locks partway, and panic sets in.
That progression isn’t random. It usually traces back to one small structure slipping out of place inside the joint — and caught early, while that structure can still be saved, the problem is often treatable without replacing the joint at all.
The Real Problem: A Displaced Articular Disc
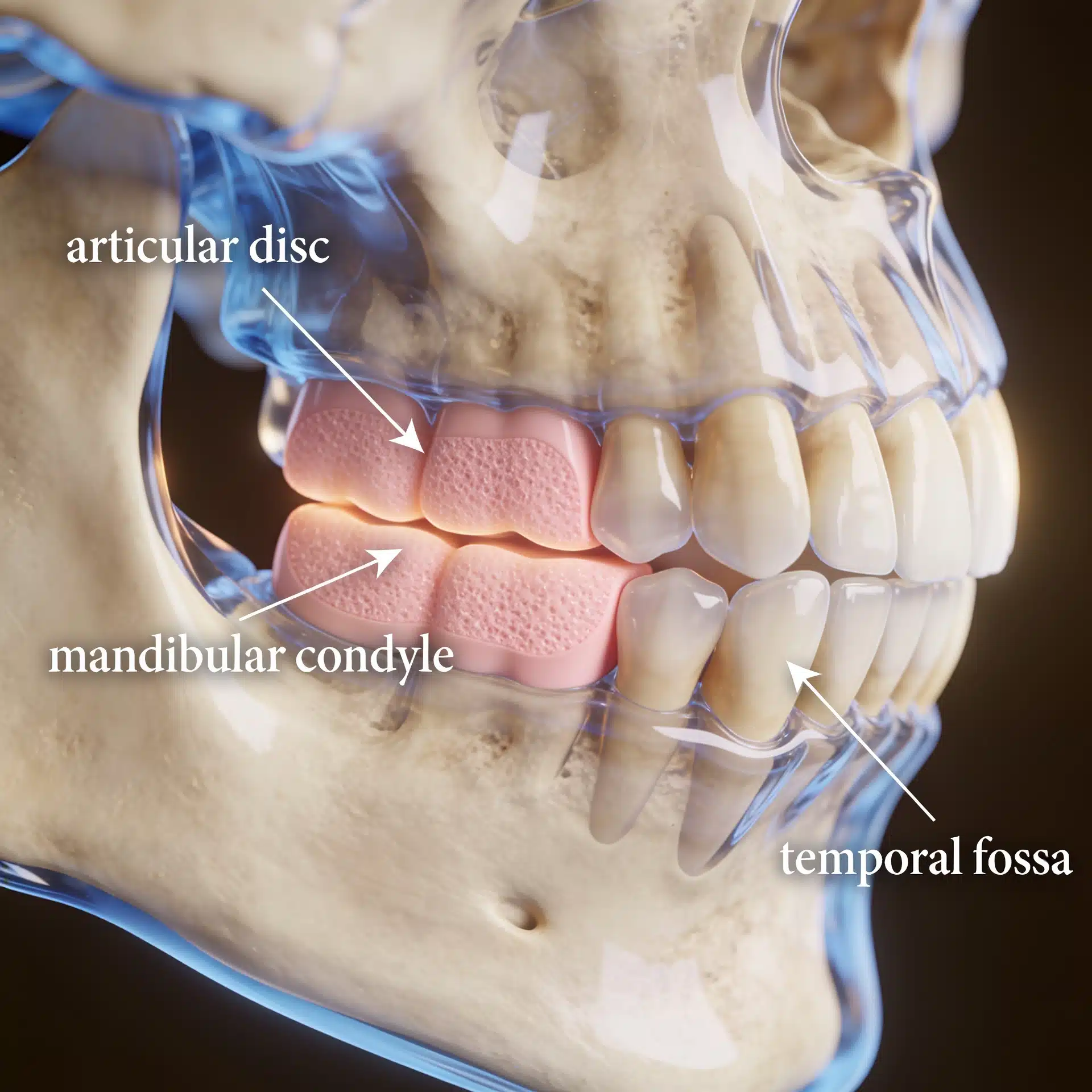
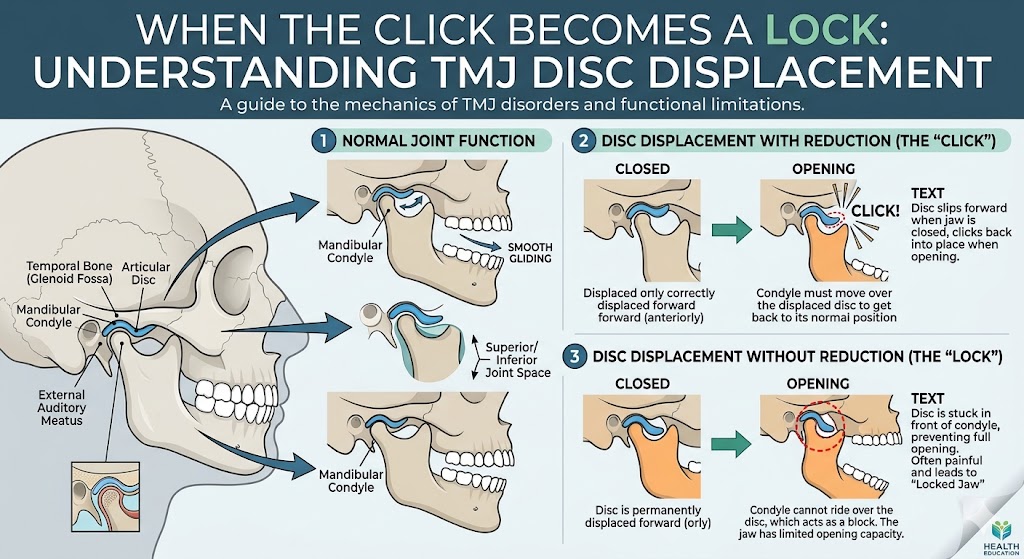
Inside each temporomandibular joint sits a small fibrocartilage disc that cushions the jaw condyle as it glides. When that disc slips forward out of position — most often anteriorly — the smooth glide is interrupted. This is called internal derangement, and it is the most common temporomandibular joint disorder.
In the early stage, the disc still snaps back into place as you open, producing the classic click (a “reducing” disc). Over time it can stop reducing — the disc stays jammed in front of the condyle, blocking full opening and causing the jaw to lock (a “non-reducing” disc). Non-reducing discs tend to degenerate and deform faster, and a chronically displaced disc can set off a cascade: inflammation, arthritis, and in some cases erosion of the condyle itself.
One point matters more than any other here, and it’s widely misunderstood: braces and jaw surgery do not, by themselves, fix a displaced disc. Moving the teeth or the jaws does nothing to put the disc back on the condyle — and in some cases, advancing the jaw onto a displaced disc makes pain and joint damage worse. The disc is its own problem, and it has to be addressed as its own problem.

What an Experienced TMJ Surgeon Brings to the Decision
The value of a focused practice here is not a promise to operate — most disc displacement is managed without surgery — but knowing when the disc can still be saved, and having a reliable way to keep it in place once it is. Older disc-repositioning surgeries had inconsistent results, often because the repositioned disc didn’t stay put: surgeons were suturing into stretched, inflamed ligaments that couldn’t hold.
To solve that, Dr. Wolford developed the Mitek Anchor technique, which secures the repositioned disc to the condyle with a small bone anchor and artificial ligaments rather than relying on damaged tissue. He has performed more of these procedures than any surgeon in the country and has authored over 185 peer-reviewed publications, including studies documenting the long-term stability the technique provides. That experience doesn’t change your joint — but it changes the odds that, if surgery is warranted, the disc stays where it’s put. (The practice’s overview of displaced articular disc disorder explains the condition in more detail.)
Key Takeaways
- A displaced articular disc (internal derangement) is the most common TMJ disorder — and the usual reason for clicking, catching, and locking.
- Most cases are managed without surgery. Conservative care comes first.
- Timing matters. A “reducing” disc that still clicks is earlier-stage than a “non-reducing” disc that locks; non-reducing discs degenerate faster.
- Braces and jaw surgery don’t fix a displaced disc. The disc is a separate problem requiring its own treatment.
- When surgery is warranted and the disc is salvageable, repositioning and stabilizing it (Mitek Anchor technique) can restore a stable, functioning joint without replacement.
- Goals are realistic: reduce pain, restore opening and function, and protect the joint from further damage. Outcomes vary and are never guaranteed.
How the Decision Is Actually Made
Short answer: Treatment escalates only as far as it needs to — conservative care for most patients, joint-sparing disc repositioning when the disc can still be saved and symptoms persist, and total joint reconstruction reserved for joints that are already beyond salvage.
Here is the reasoning behind that answer.
Diagnosis depends on imaging the disc, not just the symptoms. Clicking and pain are clues, but they don’t show disc position. An MRI is the key test — it reveals whether the disc is displaced, whether it reduces on opening, and how much degeneration has occurred. (Dr. Wolford’s overview of MRI evaluation for the TMJ explains what the imaging shows, and the National Institutes of Health offers a patient guide to temporomandibular disorders covering the broader category.)
Conservative care is the starting point for most patients. Many people with disc displacement improve with non-surgical measures. Surgery is considered when symptoms persist or progress despite appropriate conservative treatment, or when the joint is locking and function is compromised.
When surgery is indicated, the disc is repositioned if it can be saved. Patients with a salvageable disc and few or no prior joint surgeries are often good candidates for disc repositioning with the Mitek Anchor technique, frequently combined with any corrective jaw surgery needed for the bite. Published outcomes show that repositioning and stabilizing the disc adds substantial long-term stability compared with leaving it displaced. (The practice’s TMJ surgery treatment-planning page describes how these decisions are sequenced.)
Replacement is reserved for joints beyond saving. Patients with two or more prior TMJ surgeries, non-salvageable discs, or widespread joint disease tend to do better with total joint reconstruction than with repeated attempts to repair tissue that can no longer hold. Matching the procedure to the stage of disease is the whole point.
Success is defined honestly. Realistic objectives are pain reduction, restored opening and function, and protection of the joint from further breakdown. Every surgery carries risk, and a candid discussion of those risks is part of informed consent. (More on the surgical options for TMJ disorders.)
Where This Care Happens

Dr. Wolford’s practice is located on the campus of Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 — minutes from downtown Dallas and accessible from across the Dallas–Fort Worth metroplex. Valet parking is available, with self-parking in the adjacent building.
Patients travel to Dallas from across the country and internationally for TMJ evaluation, often flying into DFW or Dallas Love Field. All procedures for both current and new patients are performed exclusively at the Dallas office. Out-of-town patients can review what to bring — including any MRI or prior imaging — on the patient information page. A free initial telephone consultation is available at 214-828-9115, or you can contact the office online.
Frequently Asked Questions
Is jaw clicking always a problem? Not necessarily. Many people have painless clicking that never progresses. It becomes a concern when it’s accompanied by pain, catching, locking, or limited opening — or when the clicking changes over time.
Will my jaw definitely lock if I have a displaced disc? No. Some displaced discs remain stable for years. Others progress from clicking to catching to locking. Imaging and follow-up help determine which pattern applies to you.
Do I need surgery for a displaced disc? Most patients don’t. Conservative care is the first line, and surgery is considered only when symptoms persist or the joint is locking despite appropriate non-surgical treatment.
Why won’t braces or jaw surgery fix the clicking? Because moving the teeth or jaws doesn’t reposition the disc. If a displaced disc is contributing to symptoms, it has to be addressed directly — orthodontics and jaw surgery don’t do that on their own.
Does it matter how long I wait? Yes. A disc that still reduces (clicks) is generally earlier-stage than one that has stopped reducing (locks), and chronically displaced discs degenerate faster. Earlier evaluation gives more options while the disc may still be salvageable.
What’s the difference between disc repositioning and joint replacement? Disc repositioning saves and stabilizes your own disc — appropriate when the disc is still viable. Joint replacement reconstructs the joint with a prosthesis — reserved for joints that are already beyond repair. Which one fits depends on the condition of your joint.
About the Author
Larry M. Wolford, DMD is a board-certified oral and maxillofacial surgeon in Dallas, Texas (NPI 1821178955; National Provider Taxonomy: Oral & Maxillofacial Surgery, 1223S0112X). He earned his DMD from Temple University School of Dentistry and completed his residency in Oral and Maxillofacial Surgery at the University of Texas Southwestern Medical School in Dallas.
He is a Diplomate of the American Board of Oral and Maxillofacial Surgery and has served on its Advisory Committee, and a Clinical Professor of Oral and Maxillofacial Surgery and Orthodontics at Texas A&M University Health Science Center, Baylor College of Dentistry. His professional memberships include the American Association of Oral and Maxillofacial Surgeons, the American Society of TMJ Surgeons, the American Academy of Craniomaxillofacial Surgeons, and the American Academy of Craniofacial Pain.
Over a career spanning more than four decades, Dr. Wolford has authored over 185 peer-reviewed publications and more than 150 scientific abstracts, and holds multiple patents for surgical techniques and devices. He developed the Mitek Anchor technique for repositioning the TMJ articular disc and has performed more of these procedures than any surgeon in the country. He has trained hundreds of surgeons through fellowship programs and lectures worldwide on TMJ and orthognathic surgery.
Practice: Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 · Free initial telephone consultation: 214-828-9115
Verify credentials via the NPPES NPI Registry.
Related Reading on This Site
- What Is Displaced Articular Disc TMJ Disorder?
- Treatment Plan for TMJ Surgery
- MRI Evaluation for TMJ
- The Role of Maxillofacial Surgery in Treating TMJ Disorders
- TMJ Dysfunction: Symptoms and Treatment
- Total TMJ Replacement
- About Dr. Larry M. Wolford, DMD
- Patient Information
- Contact the Office
Authoritative Resources (External)
These independent, non-commercial sources offer further patient education:
- National Institute of Dental and Craniofacial Research (NIH): Temporomandibular Disorders (TMD) overview, which describes internal derangement and displaced discs
- American Association of Oral and Maxillofacial Surgeons (professional society): the experts in face, mouth and jaw surgery
A note on patient stories: Any patient example used in marketing for this practice should be either fully de-identified or used only with written patient authorization, consistent with HIPAA. The scenarios described in this article are general and composite, not specific patients.