Medically reviewed and authored by Larry M. Wolford, DMD — Board-Certified Oral & Maxillofacial Surgeon, Dallas, TX. Last reviewed: May 2026.
Educational disclaimer: This article is for general educational purposes and is not a substitute for an individualized medical evaluation. Whether revision surgery is appropriate can only be determined through in-person examination, records review, and imaging. No outcome is guaranteed; results vary by patient.
For a while, it looked like it worked. The braces came off, the bite lined up, the swelling went down. Then — months or years later — something shifted. The bite drifted open again. The chin slid back. Old jaw pain returned, or new pain arrived. For some patients, breathing and sleep quietly got worse. The hardest part is often the self-doubt that follows: Did I do something wrong? Is this just how it is now?
It usually isn’t. When corrective jaw surgery relapses or falls short, there is almost always a structural reason — and identifying that reason is the entire job of revision (re-do) orthognathic surgery.
Why First-Time Jaw Surgery Sometimes Fails
The problem here isn’t a villain. Revision orthognathic surgery is one of the most technically demanding areas in all of maxillofacial surgery, and even carefully performed operations can fail for reasons that were difficult to see at the time. Naming those reasons matters, because the cause dictates the fix.
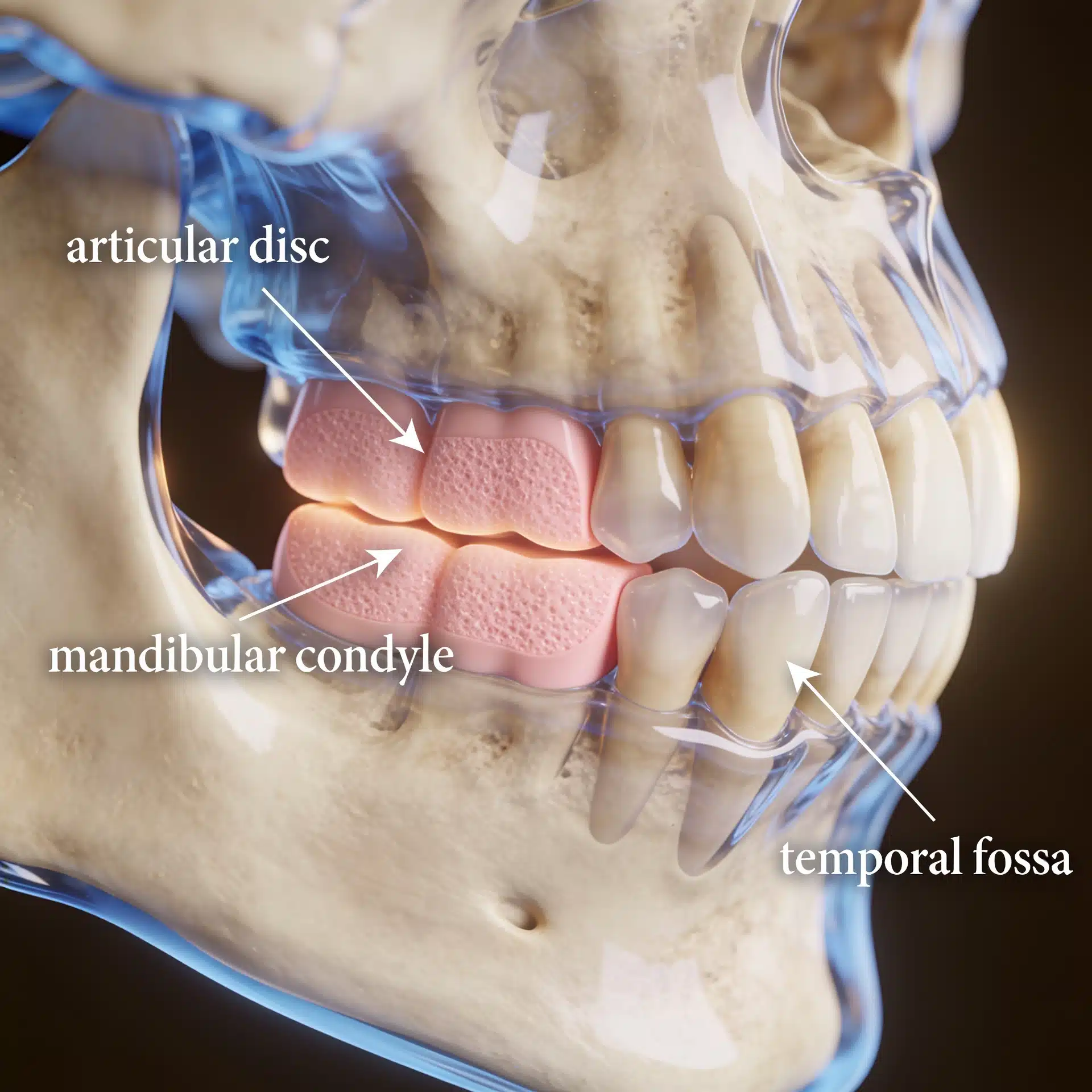
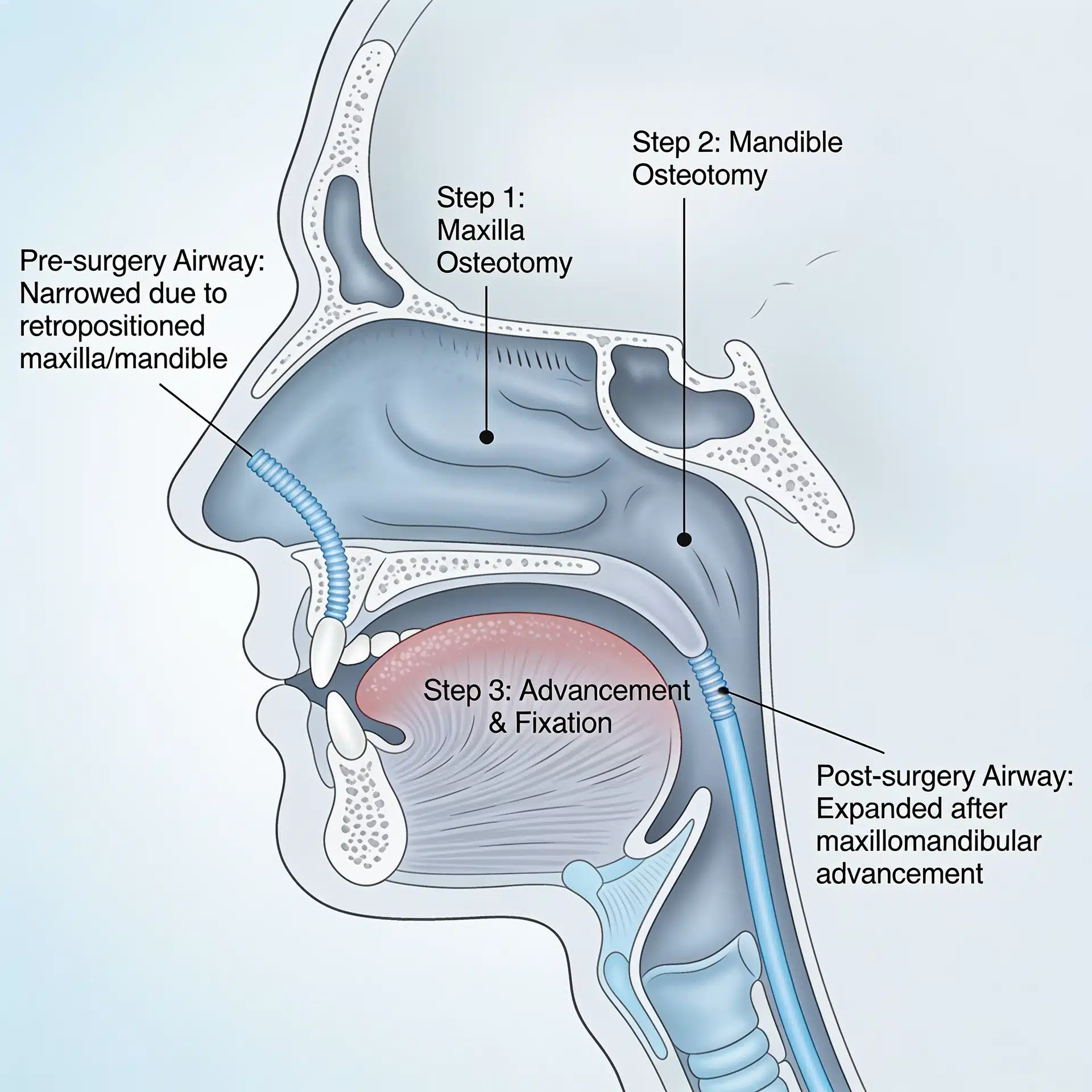
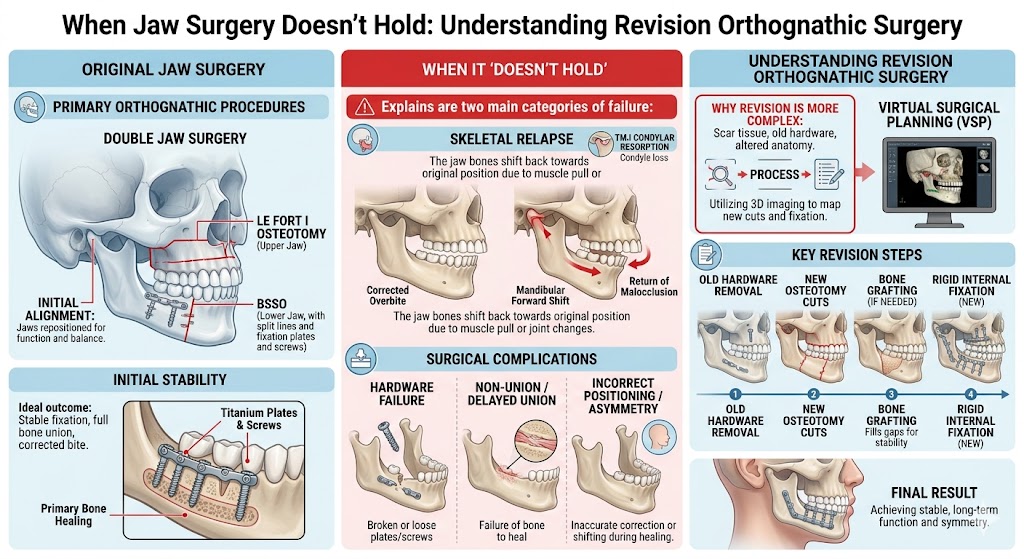
A few patterns account for most cases. The most common — and most often missed — is an unstable temporomandibular joint. When the TMJ is diseased or the jaw condyle is undergoing resorption, moving the jaws into a beautiful new position doesn’t last; the foundation keeps changing underneath. The American Association of Oral and Maxillofacial Surgeons notes that TMJ stability is central to the long-term success of orthognathic surgery, and that an accurate diagnosis must include a thorough evaluation of the joint. Other patterns include relapse from the original direction of movement, an upper or lower jaw that was under-corrected, or a setback that narrowed the airway and triggered or worsened obstructive sleep apnea.
The point is not to assign blame. It is that a result which “fell apart” usually fell apart for a discoverable, correctable reason.

What an Experienced Revision Surgeon Brings to the Decision
The value of a revision-focused practice is not a promise that everything can be undone — no ethical surgeon can promise that. The value is diagnostic depth in cases most surgeons rarely see. Most general oral surgeons don’t perform large numbers of revision cases, precisely because they’re complex, time-intensive, and frequently require correcting the bite and the joint in the same operation.
Dr. Wolford has performed more orthognathic revision surgeries than any other maxillofacial surgeon worldwide, holds patents for techniques and devices used in the field, and has authored over 185 peer-reviewed publications. He developed protocols for treating jaw misalignment and TMJ pathology in a single, coordinated surgery — the exact scenario that derails so many primary cases. That experience doesn’t guarantee your result, but it changes the quality of the diagnosis and the plan built around it. (His overview of correcting past unsuccessful jaw surgery explains the approach in more detail.)
Key Takeaways
- A relapsed or failed jaw surgery usually has a structural cause — most often an unaddressed TMJ problem, relapse, under-correction, or an airway that was compromised.
- The fix depends on the cause. Some patients need a redo of orthognathic surgery only; others need joint reconstruction and jaw surgery together.
- TMJ stability is decisive. If the joint is unstable or resorbing, moving the jaws alone tends not to last.
- Revision is harder than primary surgery and is best handled by a surgeon who performs these cases routinely.
- Imaging and records matter. Bringing scans and notes from prior surgeries makes evaluation far more productive.
- Goals are realistic: restore function, stability, bite, and often airway — not a guaranteed return to an imagined ideal.
How the Decision Is Actually Made
Short answer: Revision orthognathic surgery is recommended once the reason the first result failed is identified — and the operation is built to correct that specific cause, which sometimes means redoing the jaw surgery alone and sometimes means reconstructing the joint and the jaws together.
Here is the reasoning behind that answer.
The diagnosis starts with old records and new imaging. A productive revision evaluation reviews what was done the first time and why, alongside fresh cone-beam CT and, when the joints are in question, an MRI. This is what separates a simple relapse from an actively resorbing joint — two problems that look similar but require very different surgeries.
The cause determines the operation. If the joints are healthy and the bite simply drifted, revision may be a redo of orthognathic surgery alone — sometimes moving the jaws in a different direction than the original surgery. If the underlying driver is mandibular condylar resorption or TMJ disease, joint replacement and jaw surgery are usually performed together. For patients whose first surgery moved the lower jaw backward and worsened breathing, revision typically advances the jaws forward to enlarge the airway.
The joint and the bite are corrected together when both are involved. Treating the bite while ignoring an unstable joint is a leading reason revisions themselves fail. When end-stage joint disease is present, total TMJ replacement with simultaneous jaw correction provides stability that bite-only revision cannot reliably achieve. (For background on the joint conditions involved, see Dr. Wolford’s TMJ dysfunction overview and the National Institutes of Health’s patient guide to temporomandibular disorders.)
Prevention is part of the conversation, too. Many revisions trace back to factors that can be screened for before a first surgery. Understanding what drives the need for revision helps patients ask better questions, whether they’re facing a redo or considering jaw surgery for the first time.
Success is defined honestly. Realistic objectives are a stable bite, restored function, relief of pain, and — where relevant — an improved airway. Revision carries more complexity and risk than primary surgery, and a candid discussion of those risks is part of informed consent.
Where This Care Happens

Dr. Wolford’s practice is located on the campus of Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 — minutes from downtown Dallas and accessible from across the Dallas–Fort Worth metroplex. Valet parking is available, with self-parking in the adjacent building.
Revision patients in particular travel to Dallas from across the country and internationally, often flying into DFW or Dallas Love Field, because surgeons who handle large volumes of complex re-do cases are rare. All procedures for both current and new patients are performed exclusively at the Dallas office. Out-of-town patients can review what records and imaging to gather on the patient information page. A free initial telephone consultation is available at 214-828-9115, or you can contact the office online.
Frequently Asked Questions
Can a failed or relapsed jaw surgery actually be fixed? In most cases, yes — but only after the structural reason for the failure is identified. Revision is harder than primary surgery, and the right plan depends entirely on the underlying cause.
Why did my first surgery relapse? Common reasons include an unstable or resorbing TMJ that wasn’t addressed, relapse from the original movement, under-correction, or an airway problem. Imaging and a review of your prior records usually reveal which applies.
Will I need TMJ replacement as part of my revision? Not always. If your joints are healthy, revision may involve the jaws only. If condylar resorption or end-stage TMJ disease is driving the problem, joint reconstruction and jaw surgery are often done together for stability.
Is revision surgery riskier than the first operation? Revision is generally more complex because of prior scarring, hardware, and altered anatomy. That complexity is exactly why these cases are best handled by a surgeon who performs them routinely. Your surgeon will review the specific risks with you.
How long after my first surgery should I wait before revision? There is no single answer; timing depends on healing, whether the joint is still changing, and the cause of the problem. This is determined individually at consultation.
Will insurance cover revision orthognathic surgery? It is frequently covered when medically necessary. When surgery is recommended, the office prepares a pre-authorization letter for your insurance company. Coverage depends on your individual plan.
About the Author
Larry M. Wolford, DMD is a board-certified oral and maxillofacial surgeon in Dallas, Texas (NPI 1821178955; National Provider Taxonomy: Oral & Maxillofacial Surgery, 1223S0112X). He earned his DMD from Temple University School of Dentistry and completed his residency in Oral and Maxillofacial Surgery at the University of Texas Southwestern Medical School in Dallas.
He is a Diplomate of the American Board of Oral and Maxillofacial Surgery and has served on its Advisory Committee, and a Clinical Professor of Oral and Maxillofacial Surgery and Orthodontics at Texas A&M University Health Science Center, Baylor College of Dentistry. His professional memberships include the American Association of Oral and Maxillofacial Surgeons, the American Society of TMJ Surgeons, the American Academy of Craniomaxillofacial Surgeons, and the American Academy of Craniofacial Pain.
Over a career spanning more than four decades, Dr. Wolford has authored over 185 peer-reviewed publications and more than 150 scientific abstracts, holds multiple patents for surgical techniques and devices, and has performed more orthognathic revision surgeries than any other maxillofacial surgeon worldwide. He developed protocols for treating TMJ pathology and jaw deformity in a single coordinated operation, and has trained hundreds of surgeons through fellowship programs and lectures worldwide.
Practice: Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 · Free initial telephone consultation: 214-828-9115
Verify credentials via the NPPES NPI Registry.
Related Reading on This Site
- Failed Jaw Surgery: When You Need Revision Surgery and How to Find a Specialist
- Orthognathic Re-Surgery to Correct Past Unsuccessful Attempts
- Orthognathic Surgery: Correcting Jaw Misalignment for Good
- Preventing Orthognathic Surgery Revisions: Key Factors and Strategies
- Total TMJ Replacement
- TMJ Dysfunction: Symptoms and Treatment
- About Dr. Larry M. Wolford, DMD
- Patient Information
- Contact the Office
Authoritative Resources (External)
These independent, non-commercial sources offer further patient education:
- American Association of Oral and Maxillofacial Surgeons (professional society): Corrective jaw (orthognathic) surgery overview, the role of joint stability in orthognathic surgery, and recovery from orthognathic surgery
- National Institute of Dental and Craniofacial Research (NIH): Temporomandibular Disorders (TMD) overview
- U.S. Food and Drug Administration: Temporomandibular Joint (TMJ) Implants (relevant when revision includes joint reconstruction)
A note on patient stories: Any patient example used in marketing for this practice should be either fully de-identified or used only with written patient authorization, consistent with HIPAA. The scenarios described in this article are general and composite, not specific patients.