Most jaw surgery patients heal beautifully and never look back. But a smaller, often overlooked group of patients ends up worse than where they started — relapsed bite, chronic pain, joint damage that wasn’t there before surgery, breathing problems that emerged afterward, or a face that doesn’t look like theirs anymore. These patients usually feel invisible in the system. The original surgeon may not be willing or able to redo the work, second opinions disagree, and information online tends to assume that surgery either works perfectly or doesn’t happen at all.
It does happen. And in many cases, it can be fixed. Complex orthognathic revision surgery is its own field within maxillofacial surgery — and it’s the field Dr. Wolford has built much of his career around.
Why does jaw surgery fail in the first place?
Failed jaw surgery isn’t usually one mistake. It’s typically a combination of factors that, taken together, produce an unstable or unhealthy result. The most common causes include:
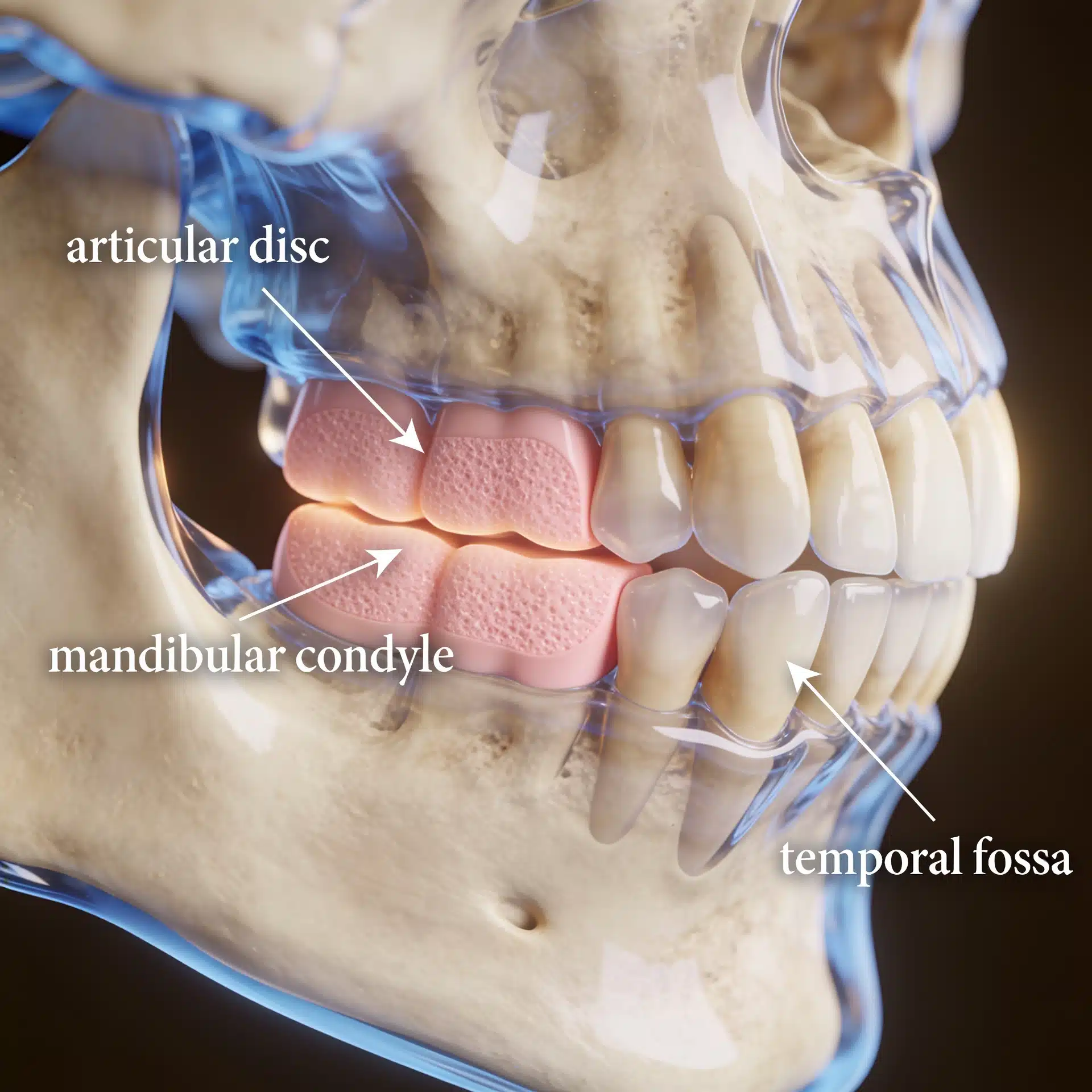
- Untreated TMJ disease at the time of surgery. If the joint is sick, no jaw surgery built on top of it will be stable. The joint will continue to change, and so will the bite. This is one of the most frequent causes of relapse.
- Inadequate surgical planning. Two-dimensional planning, no airway analysis, no joint imaging, or no consideration of facial balance often produces a result that looks acceptable on paper and fails in real life.
- Wrong direction of movement. Setting the lower jaw back to close an open bite, for example, can compress the airway and trigger sleep apnea or worsen TMJ disease.
- Hardware problems. Failed plates, screws, or older alloplastic joint implants that have broken down over time.
- Condylar resorption after surgery. Some patients lose bone in the jaw joints in the months or years after surgery, often related to undiagnosed underlying joint pathology.
Many of these problems trace back to one root issue: the temporomandibular joint and the bite were treated as if they were independent. They aren’t. The relationship between them is detailed throughout the diagnosis and treatment planning section.
Signs your previous jaw surgery didn’t fully succeed
Some signs are obvious. Others can be subtle and develop over years. Common indicators include:
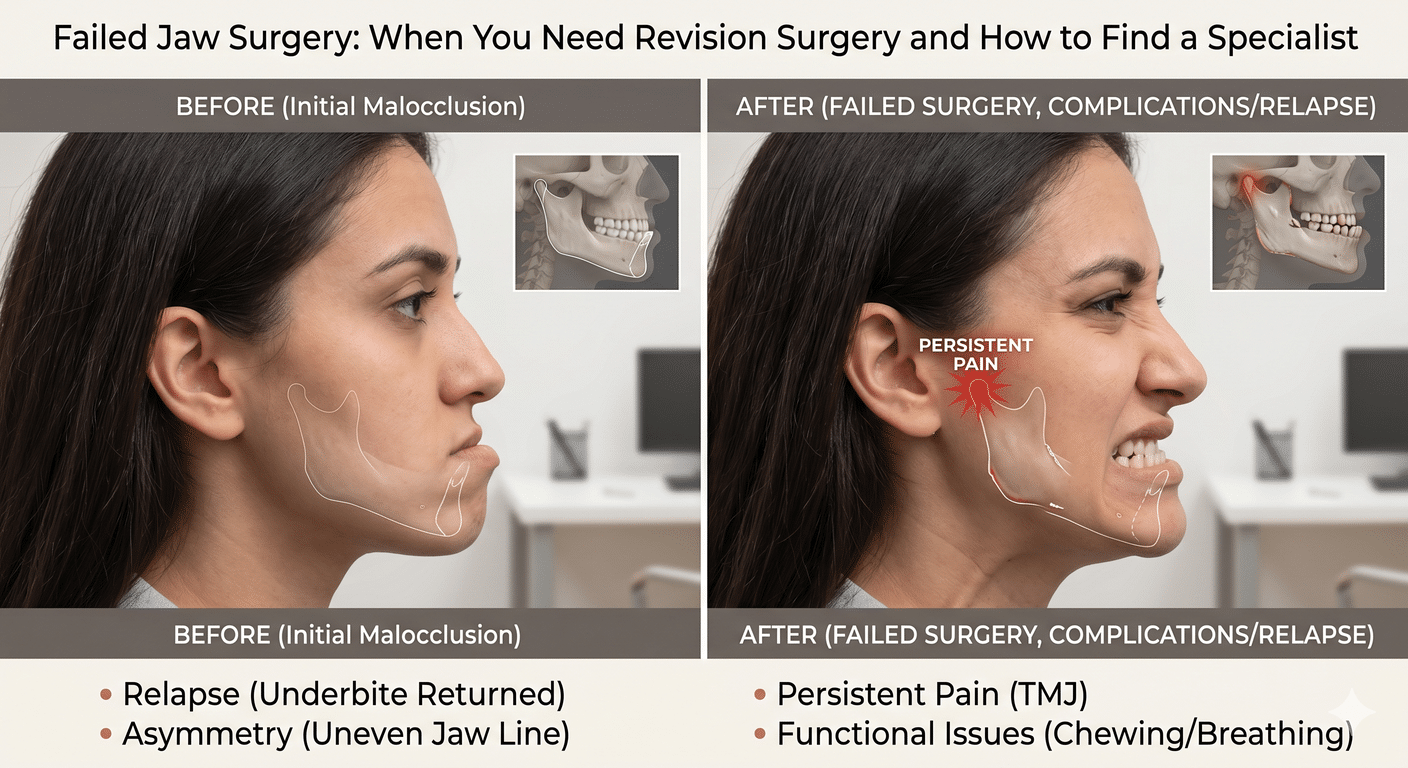
- Your bite has shifted back toward where it was before, or into a new malocclusion
- New or worsening jaw pain, headaches, or ear pain
- Limited opening or new clicking and locking
- Snoring, waking up gasping, or new daytime fatigue
- A receding chin, asymmetry, or a face that no longer looks balanced
- Numbness that didn’t improve, or new numbness
- Hardware that you can feel or that seems to be moving
If any of those describe your situation, the next step is a comprehensive workup — typically including MRI of the TMJ, 3D CT, an airway evaluation, and a thorough orthognathic surgery evaluation.
Can revision surgery actually fix it?
In most cases, yes — but the planning has to be different. Revision orthognathic surgery isn’t just “redoing” the first surgery. It’s a fundamentally different operation, because the surgeon is now working through scarred tissue, around old hardware, and on bone and joint structures that have already been altered.
A successful revision generally requires:
- Treating the joint and the bite at the same time. If the TMJ is part of why the first surgery failed, it has to be addressed in the revision — sometimes with disc repositioning, sometimes with total joint replacement.
- 3D virtual surgical planning. Modern revision cases are planned virtually before they’re performed.
- Custom hardware where appropriate. For patients needing joint replacement, patient-specific implants are now the standard of care.
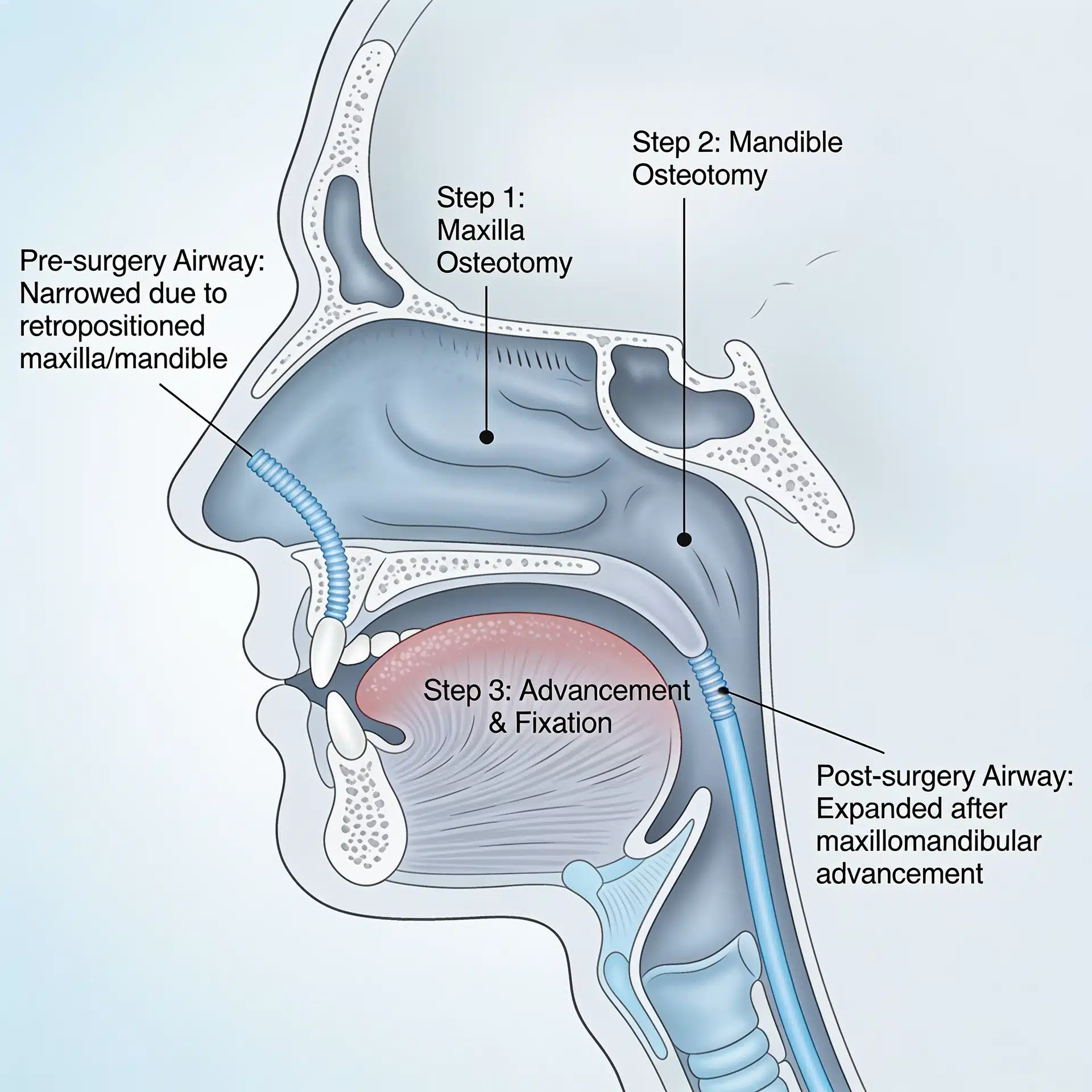
- An airway-conscious approach. Direction of movement matters as much as amount of movement, especially in patients with airway compromise.
More on the modern planning workflow is available on the virtual surgical treatment planning page.
Common revision scenarios
Bite relapse with stable joints
If the joints are healthy but the bite has drifted back, revision is often a redo of orthognathic surgery only — sometimes with a different direction of movement than the original surgery.
Bite relapse caused by ongoing condylar resorption
If the underlying problem is mandibular condylar resorption — including conditions like adolescent internal condylar resorption or TMJ disease related to autoimmune conditions — joint replacement and orthognathic surgery are usually performed together.
Sleep apnea that emerged or worsened after the first surgery
Patients whose original surgery moved the lower jaw backward often develop or worsen OSA. Revision typically involves advancing the jaws forward to enlarge the airway.
End-stage TMJ pathology after multiple prior surgeries
For patients who have had several joint surgeries already, end-stage TMJ pathology often calls for total TMJ replacement with simultaneous correction of the jaws.
How to find the right revision surgeon
Revision orthognathic surgery is one of the most technically demanding fields within maxillofacial surgery. Most general oral surgeons don’t perform large numbers of revision cases, and reasonably so — they’re complex, time-intensive, and often involve simultaneous joint and bite correction.
When evaluating a revision specialist, look for:
- High volume of revision and joint replacement cases (not just primary jaw surgery)
- Routine use of 3D virtual surgical planning
- Combined TMJ and orthognathic surgery in a single operation when appropriate
- Experience treating connective tissue and autoimmune-related joint disease
- A track record of patients traveling in from out of state and internationally
The practice’s patient testimonials and before-and-after gallery include many revision cases. The travel information page is built specifically for out-of-area revision patients.
The bottom line
If your first jaw surgery didn’t deliver what you hoped — or if the result was acceptable for a while and has slowly fallen apart — you’re not stuck. Revision is harder than primary surgery, but in experienced hands, the results can be life-changing.
To start the process, call 214.828.9115 for a free 15-minute telephone consultation, or send a message. For patients with imaging and records from prior surgeries, sharing those in advance helps make the consultation more productive.