Continuous positive airway pressure — CPAP — is the standard treatment for obstructive sleep apnea, and for many people, it works well. But a meaningful percentage of patients can’t tolerate the mask, the noise, the dryness, or the lifestyle limitation. The National Heart, Lung, and Blood Institute estimates that millions of Americans have OSA, and a significant portion of them either don’t use CPAP consistently or never start it at all.
For those patients, sleep apnea corrective surgery — particularly maxillomandibular advancement — isn’t a last resort. In the right candidate, it’s a definitive cure rather than a nightly management strategy.
Why CPAP isn’t always the right long-term answer
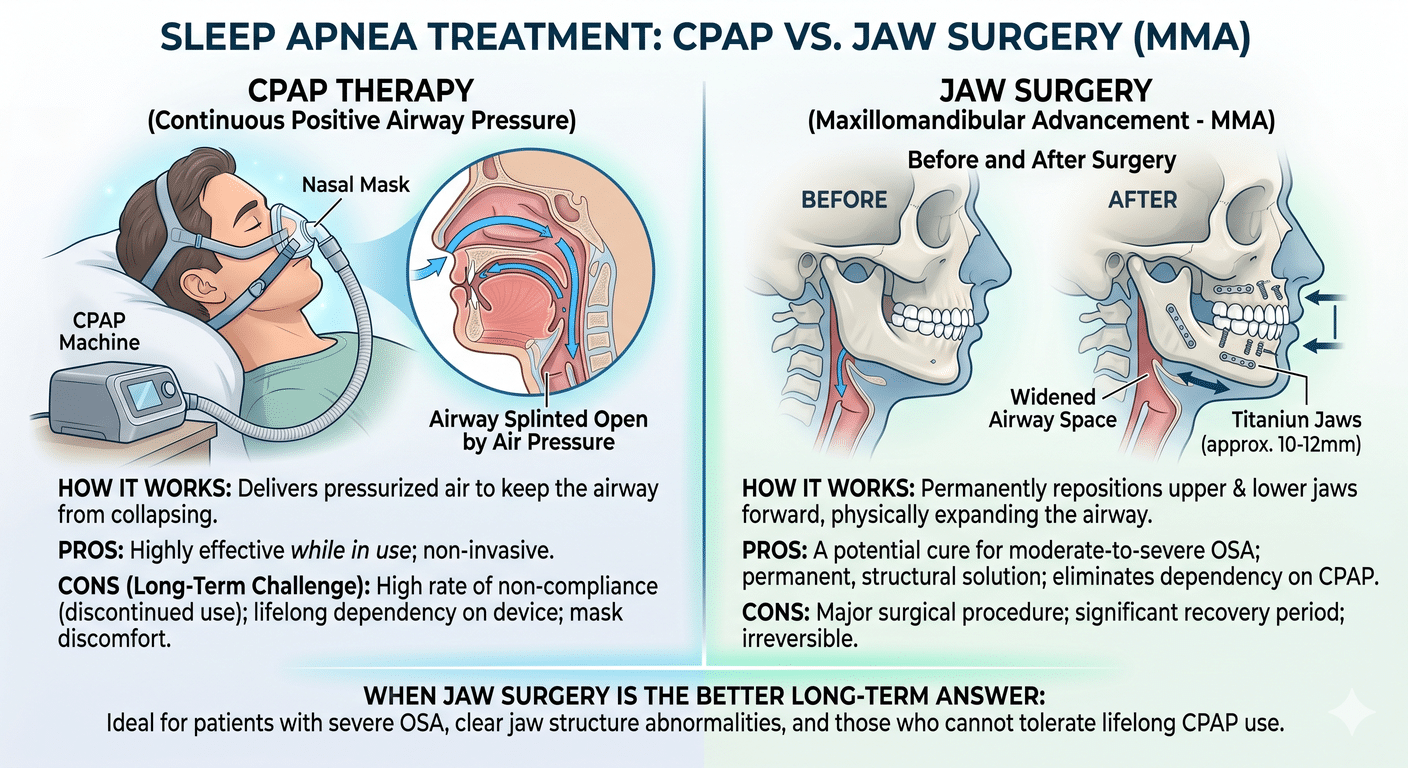
CPAP is excellent at treating the symptom — collapsed airway during sleep — but it doesn’t address why the airway is collapsing in the first place. For many patients, the underlying cause is simple anatomy: the upper and lower jaws are positioned too far back, which crowds the tongue and soft palate into the airway. CPAP forces the airway open with pressurized air. Surgery actually moves the bones forward so the airway is bigger to begin with.
Common reasons patients give up on CPAP include:
- Mask problems are a constant battle — leaks that wake you up, straps that dig in, and a creeping sense of claustrophobia that some people never fully shake. Skin irritation along the nose bridge and cheeks is common too.
- Travel becomes a hassle, and sharing a bed with a partner while strapped to a humming machine can put real strain on intimacy and sleep quality for both people.
- The physical side effects pile up: a parched mouth in the morning, stuffy sinuses, or a belly full of swallowed air (aerophagia) that leaves you bloated and uncomfortable.
- Perhaps most discouraging — some patients hit every compliance metric their doctor cares about and still wake up exhausted, which makes it hard to justify staying the course.
- Simply not wanting to be tethered to a machine for the next 40 years
According to the CDC, leaving sleep apnea untreated has been linked to a range of serious problems, including high blood pressure, heart disease, stroke, type 2 diabetes, depression, and a higher risk of car crashes. Walking away from CPAP without lining up another treatment first isn’t a small choice — it’s a real medical decision, and one worth making with a clinician rather than on your own.
Learn more from the CDC: https://www.cdc.gov/heart-disease/about/sleep-and-heart-health.html
What is maxillomandibular advancement (MMA)?
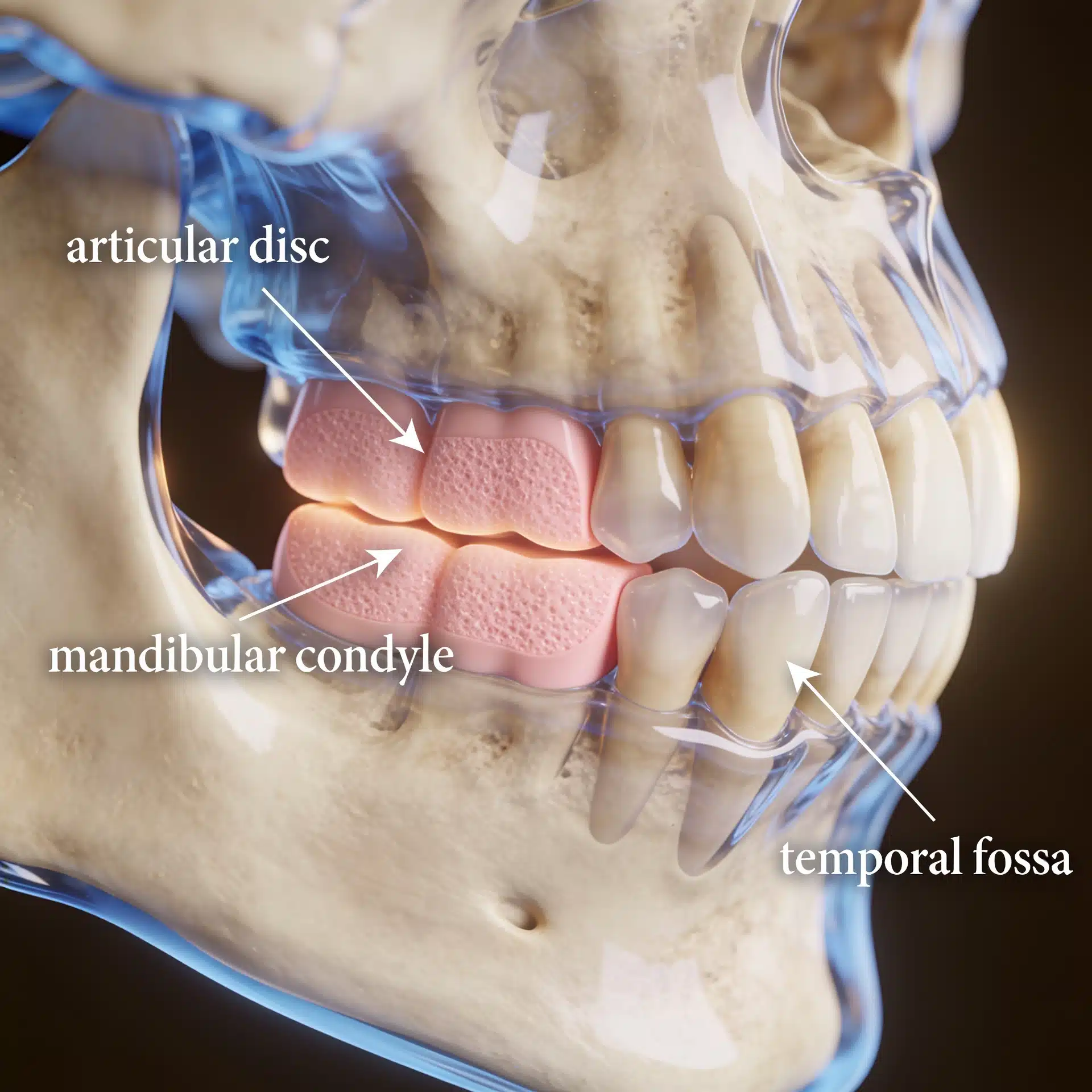
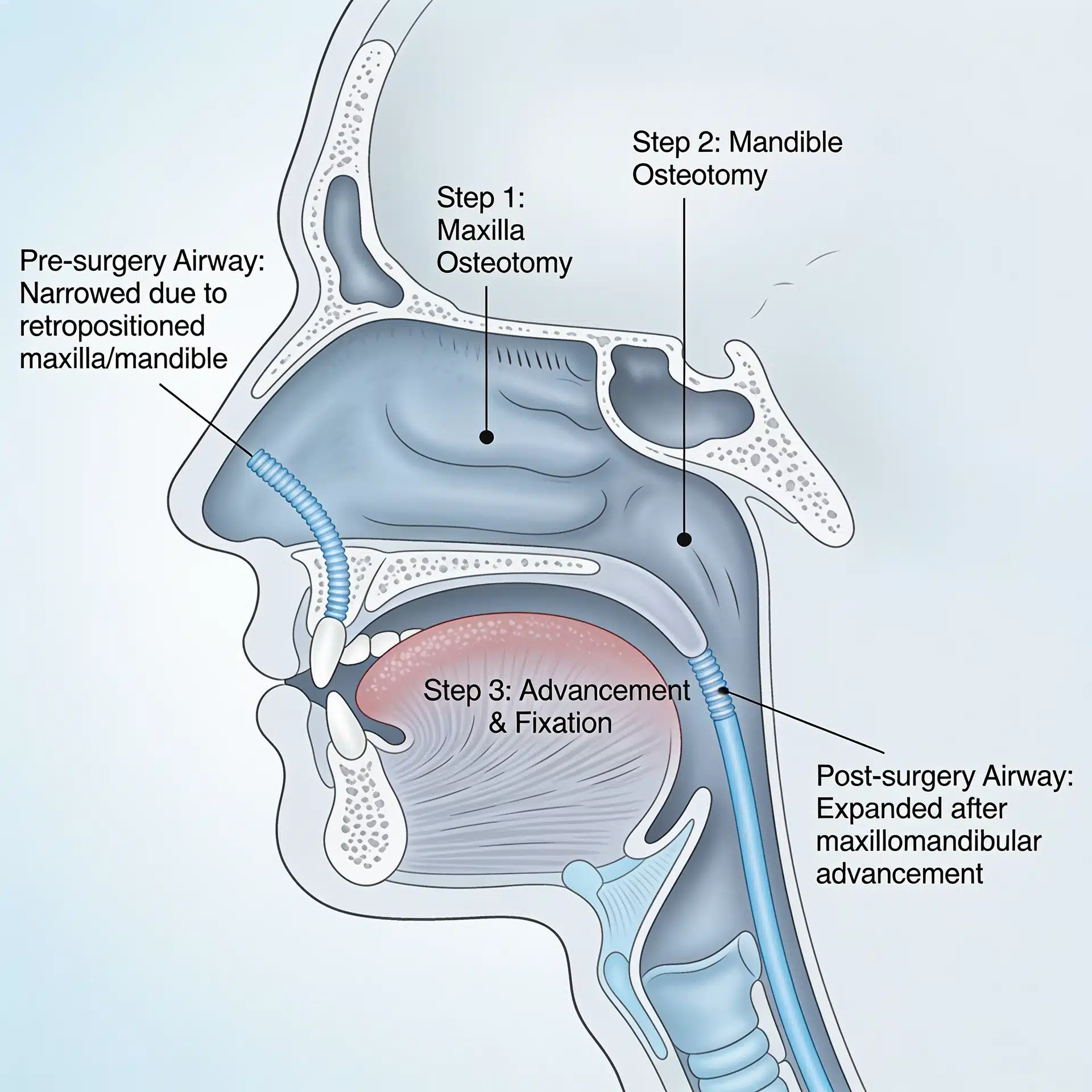
Maxillomandibular advancement is a form of orthognathic surgery that moves the upper jaw (maxilla) and lower jaw (mandible) forward, typically by 8 to 12 millimeters. As the bones move forward, the soft tissues attached to them — including the tongue base and soft palate — also move forward. The end result is a larger, more stable airway that doesn’t collapse during sleep.
It’s worth being clear about what MMA actually is. People sometimes lump it in with cosmetic jaw surgery because the face does tend to look better afterward, but that’s a side effect, not the point. The procedure is structural — surgeons move the upper and lower jaw forward to physically open up the airway behind the tongue and soft palate, so it doesn’t collapse during sleep.
For someone with severe obstructive sleep apnea who simply can’t get along with CPAP (and that’s a lot of people — the mask, the pressure, the noise, the claustrophobia), the options narrow quickly. MMA is one of the few interventions that actually shows durable cure rates years out from surgery, not just symptom management.
How effective is jaw advancement for sleep apnea?
Published research, including studies authored by Dr. Wolford and colleagues, has shown that MMA produces significant and stable airway improvements. Several of the relevant studies are listed on the practice’s research publications page, including work on airway space changes after double orthognathic surgery and the effects of double orthognathic surgery on OSA.
In appropriately selected patients, MMA has consistently been shown in the medical literature to be one of the most effective surgical treatments for OSA, often producing outcomes that approach or rival CPAP — but without the nightly device. The American Academy of Sleep Medicine recognizes maxillomandibular advancement as a treatment option for moderate to severe OSA in selected patients.
Who is a good candidate for jaw advancement surgery?
Not everyone with OSA needs jaw surgery, and not everyone with OSA is a good candidate for it. Generally, the best candidates share several features:
- You’ve had a sleep study that shows moderate or severe sleep apnea
- CPAP hasn’t worked for you, whether that’s because it’s uncomfortable or just isn’t doing the job
- Your upper or lower jaw sits further back than it should, or your lower face is on the smaller side
- Imaging shows your airway is narrow
- You’re in good enough shape for surgery
Some patients also have an underlying jaw or bite problem that has been quietly causing both their OSA and other symptoms — including TMJ dysfunction or chronic facial pain. In those patients, addressing the bite, joint, and airway together can change everything.
The first step in candidacy is a thorough airway evaluation for TMJ and orthognathic surgery. Patients can also start by completing the airway questionnaire for obstructive sleep apnea.
What recovery actually looks like
Most patients spend one to two nights in the hospital after surgery. Swelling peaks in the first week and is largely gone by week three to four. Patients are on a non-chew diet for several weeks, then transition gradually back to normal foods. Most people return to desk work in two to three weeks and to full activity by six to eight weeks.
Detailed expectations and post-surgical guidelines are available on the postoperative instructions page, and travel logistics for out-of-town patients are outlined on the travel information page.
CPAP vs. surgery: how to think about the decision
Neither CPAP nor surgery is the right answer for everyone. CPAP isn’t invasive, you can stop using it anytime, and it works well if you actually wear it. Surgery is a one-shot fix that changes the underlying structure and can be curative in the right cases. What’s right for you comes down to a few things: how severe your OSA is, what your anatomy looks like, whether CPAP is genuinely working when you use it, your age and overall health, and how much it matters to you not to be hooked up to a machine every night.
If you’re tolerating CPAP and your apnea is well controlled, there’s no reason to switch. If you’ve tried CPAP for months or years and you still feel exhausted, still snore, or simply can’t keep using it — surgery is worth a real conversation.
The bottom line
Sleep apnea kills slowly. It also wrecks daily life — relationships, work performance, mood, and metabolic health. CPAP saves lives when patients can use it. For the patients who can’t, jaw advancement surgery can be a permanent answer rather than a nightly battle.
To find out whether you’re a candidate, call 214.828.9115 for a free 15-minute telephone consultation, or request an evaluation.