If you’ve been anywhere near TikTok, Instagram, or YouTube in the past year, you’ve seen the vocabulary: mewing, looksmaxxing, hunter eyes, canthal tilt, bone smashing, hardmaxxing, softmaxxing. What started on niche forums as a cluster of grooming and skincare tips has exploded into a full-blown cultural movement, particularly among young men. Search interest for the term “looksmaxxing” jumped more than 30% in early 2026, and the trend now encompasses everything from legitimate self-improvement to genuinely dangerous DIY facial modification.
Those of us who operate on the jaw and midface for a living are seeing the downstream effects of looksmaxxing in our consult rooms, and the trend raises legitimate clinical concerns. Patients, many of them in their late teens and twenties, arrive with self-diagnoses drawn from TikTok, curated photo references of jawlines they want to replicate, and a set of expectations that range from reasonable to structurally impossible. What a sixty-second video compresses into a confident recommendation is almost always more complex in practice.
This article lays out what looksmaxxing actually refers to, which elements of it have support in the medical literature, which cross into outright misinformation, and how genuine orthognathic surgery fits into the broader conversation. A meaningful subset of patients drawn to the trend do have real skeletal or occlusal issues that warrant formal evaluation, and they deserve a careful workup rather than a reflexive dismissal. The aim here is to draw a clear line between structural problems that respond to surgical correction and cosmetic concerns manufactured by an algorithm.
What Looksmaxxing Actually Is
Looksmaxxing is an umbrella term for maximizing one’s physical attractiveness — and the community that has grown around it online has developed a surprisingly specific internal taxonomy. Softmaxxing refers to the safer entry points: skincare, hairstyling, fitness, grooming, and sleep hygiene. Hardmaxxing refers to invasive interventions, including cosmetic surgery, jaw implants, and genuinely dangerous practices like “bone smashing.”
In between sits a middle tier where most of the viral content actually lives: mewing, jaw exercises, chewing hard gum, mastic gum routines, facial massage tools, and various posture interventions. Some of these are benign. Some are pointless. And some are actively harmful.
The cultural underpinning is what makes this different from previous appearance-obsession waves. In 2026, AI filters, beauty apps, and hyper-visual social feeds have created an environment in which young users are comparing themselves not to real peers but to digitally optimized versions of strangers. Plastic surgeons are reporting that the trend is most visible in young men in their 20s, and mental health professionals have begun flagging the rise as a driver of body dysmorphia, anxiety, and social comparison-based depression.
Mewing: The Most Famous, Most Misunderstood Piece of the Trend
Mewing — named after the British orthodontists John and Michael Mew — is the practice of resting the tongue flat against the palate, with the tip behind the upper incisors. The theory is that consistent tongue pressure reshapes the jaw and midface over time, producing a more defined jawline and better facial structure.
The medical consensus on mewing is clearer than the TikTok conversation suggests. The American Association of Orthodontists does not recommend mewing and has cautioned that the claims about reshaping the adult jawline through tongue posture are not supported by scientific evidence. Board-certified oral and maxillofacial surgeons have been even blunter: there is no credible medical evidence that mewing can reshape the jawline or facial structure, particularly past early childhood. Once facial growth is complete, bones are not meaningfully malleable in response to soft-tissue pressure from the tongue.
A few important nuances are worth preserving, though:
- Tongue posture does matter in childhood facial development. The Mews did not invent this observation, and it’s genuinely accepted in the orthodontic literature that tongue posture, oral breathing, and airway patency influence how the face develops during growth. This is the kernel of legitimate science the mewing community has wrapped in exaggerated claims.
- Tongue thrust is a real thing. Some patients do have tongue-thrust patterns that shift teeth and worsen certain malocclusions. That’s an appropriate reason to see an orthodontist — not a reason to spend two years pressing your tongue against the roof of your mouth hoping to grow a new jawline.
- “Before-and-after” mewing photos are almost always lighting, angle, facial hair, posture, and weight loss. The same face photographed from above with a neutral expression looks radically different from a face photographed from below with a clenched jaw. Most mewing transformations are being produced by the camera, not the tongue.
John Mew was stripped of his dental license years ago, and his son Michael has faced misconduct proceedings at the General Dental Council. That context matters — not as a gotcha, but because the intellectual foundation for a multi-billion-view trend was produced by practitioners operating well outside the mainstream of orthodontic medicine.
“Bone Smashing” and the Truly Dangerous End of the Trend
At the far end of the looksmaxxing spectrum sits “bone smashing” — the genuinely alarming practice of striking one’s own cheekbones, jaw, or chin with a hammer or other blunt instrument, based on a misinterpretation of Wolff’s Law (the idea that bone remodels in response to mechanical stress).
The claim is that repeated micro-trauma causes the bone to rebuild itself denser and more prominent. The reality is that Wolff’s Law describes the gradual remodeling of bone under controlled physiologic loading — the kind produced by muscular contraction during normal activity, not blunt-force trauma. Hitting your face with a hammer doesn’t trigger productive remodeling. It produces contusions, microfractures, soft-tissue damage, and — in a growing number of reported cases — genuine facial fractures requiring emergency maxillofacial repair.
The looksmaxxing community’s taxonomy also includes elective jaw implant surgery, cheekbone implants, orbital reshaping, and chin augmentation, much of which is sought overseas in medical-tourism hubs. Mental health professionals continue to warn that the extreme expressions of the trend act as catalysts for body dysmorphic disorder and severe anxiety, and the trend has already produced at least one high-profile hospitalization of a looksmaxxing influencer during a livestream.
Where Legitimate Jaw Surgery Actually Fits
Here’s the uncomfortable reality that gets lost in both the “anti-mewing” pushback and the pro-looksmaxxing evangelism: some of the young people drawn to this trend genuinely do have jaw structure issues that warrant medical evaluation.
The human jaw has, in fact, gotten smaller over the past several generations. Oral surgeons with decades of experience broadly agree that this change is too rapid to be evolutionary and is instead driven by lifestyle factors — softer diets, early bottle-feeding, mouth breathing, chronic nasal obstruction, and loss of prolonged breastfeeding during infancy. The downstream consequences are real: more crowded teeth, more impacted third molars, narrower dental arches, more retruded mandibles, and — increasingly — more obstructive sleep apnea in young adults who look otherwise healthy.
A subset of patients who discover “mewing” on TikTok and become convinced they need a more defined jawline are actually perceiving something real about their own anatomy. They have retruded mandibles, compromised airways, narrow arches, or dental-skeletal discrepancies that have been present since adolescence and were never diagnosed. For this group, orthognathic (corrective jaw) surgery is a legitimate, life-changing option — but it’s a medical decision, not an aesthetic one.
The distinction matters. Orthognathic surgery is performed to correct:
- Significant skeletal malocclusion (open bite, severe overbite, severe underbite, crossbite) that cannot be addressed with orthodontics alone
- Retrognathic mandibles producing chronic airway compromise or confirmed obstructive sleep apnea
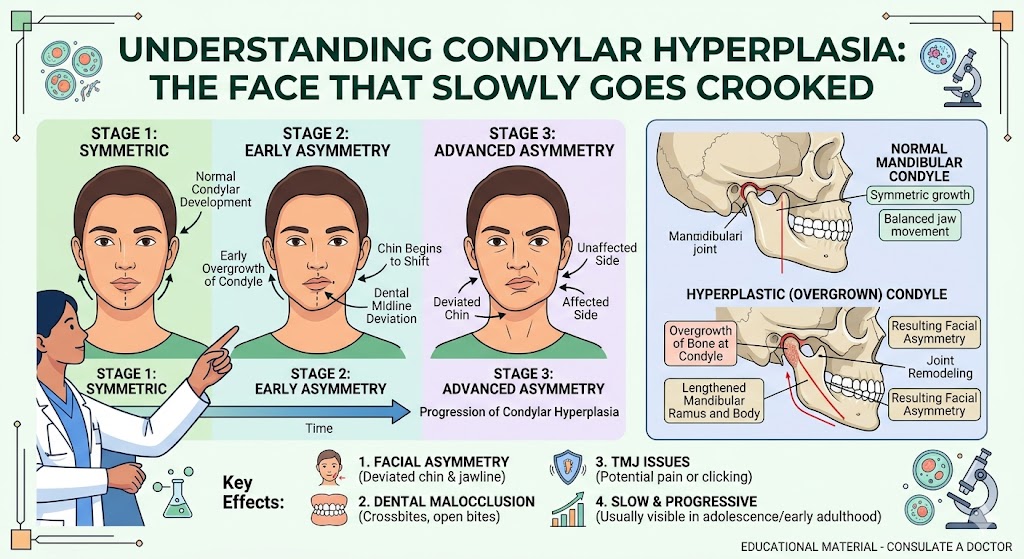
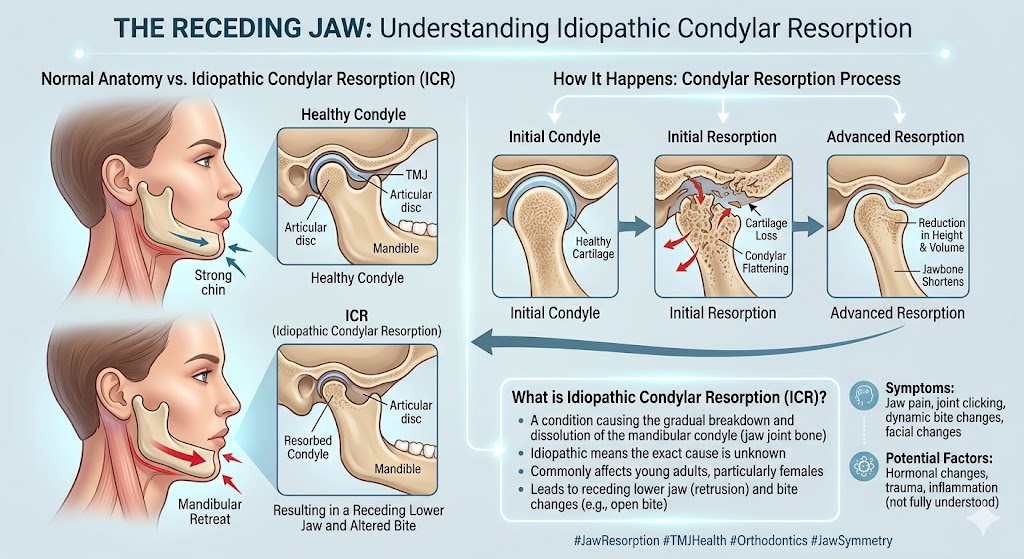
- Mandibular asymmetry, including condylar hyperplasia and related growth disorders
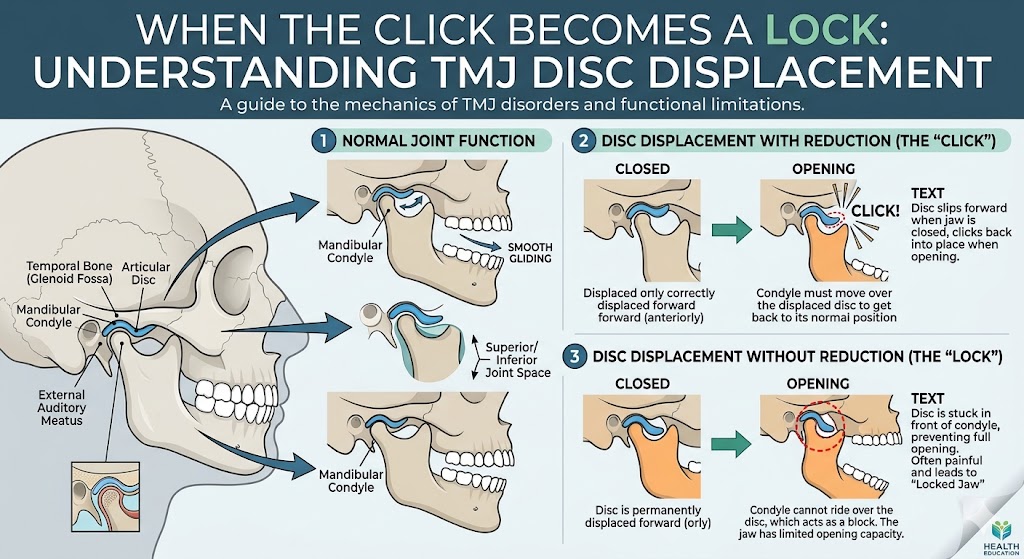
- TMJ disease coexisting with jaw deformity, which often requires concomitant TMJ and orthognathic surgery
- Craniofacial deformities and syndromic presentations
- Failed prior orthognathic surgery requiring complex revision
When orthognathic surgery is performed for the right indications, the outcomes are extraordinary — not just functionally but psychologically. A 2025 retrospective study of 60 orthognathic surgery patients found significant improvements in quality of life, self-esteem, body image, and emotional stability after surgery. A broader recent review of current trends in orthognathic surgery noted that advances in computer-assisted planning, patient-specific fixation, and airway-oriented treatment protocols have made outcomes more predictable than at any point in the field’s history.
The patients who benefit most, though, are evaluated honestly — by a surgeon who will tell them when surgery is the right answer and when it isn’t.
Why Looksmaxxing-Driven Patients Need Especially Careful Evaluation
A patient who arrives at a maxillofacial consultation because their bite is destroying their molars, their condyles are resorbing, or their airway collapses every night during sleep is a fundamentally different patient from one who has spent six months watching TikTok videos and has decided they need a more defined jawline.
Both patients deserve respect and honest evaluation. But they require different conversations.
For the first patient, the clinical task is straightforward: diagnose the pathology, plan the surgery, and execute it. For the second, the clinical task is more nuanced. A good surgeon has to assess whether there’s a legitimate underlying skeletal or airway issue that the patient has correctly sensed even if they’ve misnamed it — and, equally importantly, whether the patient’s expectations are grounded in reality or shaped by filtered images and online communities promoting an impossible standard.
A few principles that guide how serious maxillofacial practices approach this growing population:
A thorough diagnostic workup comes first — every time. Before any conversation about surgery, patients should receive a full evaluation for dentofacial deformity, including cephalometric imaging, an airway assessment, a TMJ evaluation, and a functional occlusal analysis. A patient who walks in asking about “jaw forward surgery” may turn out to have a significant Class II skeletal pattern with previously undiagnosed sleep apnea — a surgical case with strong medical indications. Or they may have a cosmetically normal profile and a well-functioning bite, in which case surgery is not the appropriate path.
Screening for body dysmorphic disorder is a real part of responsible practice. Mental health professionals now consistently warn that looksmaxxing and similar appearance-obsession trends can drive or reveal underlying body dysmorphic disorder. Reputable surgeons will defer or decline elective facial surgery in patients whose expectations don’t match observable reality, or whose distress isn’t going to be resolved by bone movement.
Virtual surgical planning has made realistic preview possible. Virtual surgical treatment planning now allows patients to see accurate, anatomically grounded simulations of proposed surgical movements — not TikTok-filter fantasies, but honest three-dimensional projections of what their face will look like afterward. This is one of the most important advances of the last decade for managing expectations.
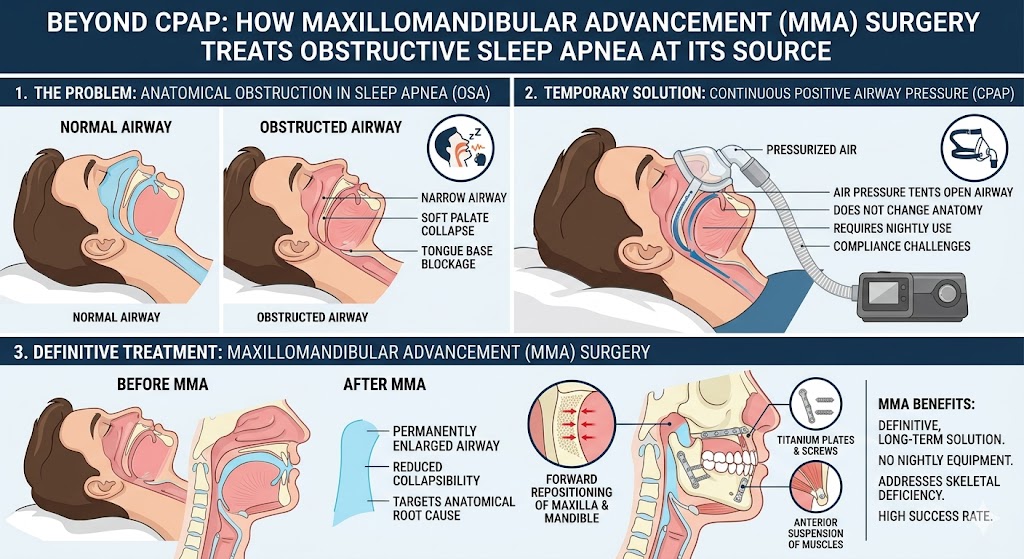
The airway should drive the plan, not the jawline. One of the underappreciated lessons of the last twenty years of orthognathic surgery research is that jaw movements that enlarge the airway tend to produce both functional and aesthetic improvement. Maxillomandibular advancement for obstructive sleep apnea repositions both jaws forward, expands the airway, treats snoring and apnea — and, as a secondary effect, produces a more defined facial profile. When the airway is treated properly, aesthetics tend to follow. The reverse — chasing aesthetics and ignoring the airway — produces inferior results and sometimes worsens sleep-disordered breathing.
A Simple Framework for Young People Drawn to the Trend
If you’re a younger reader who landed here because you’ve spent time in looksmaxxing communities and you’re trying to figure out what’s legitimate and what isn’t, a few filters are worth applying:
If a technique promises to reshape adult bone without surgery, it is almost certainly overstated. Tongue posture, chewing hard foods, and facial exercises do not meaningfully change the adult facial skeleton.
If a technique involves blunt trauma, it is dangerous. Full stop. Hitting your face with objects does not produce productive bone remodeling; it produces injuries.
If you genuinely have symptoms — chronic fatigue despite adequate sleep, observed snoring or gasping at night, jaw pain, clicking, limited opening, a bite that doesn’t close properly, or facial asymmetry — you’re in a different category. Those symptoms deserve a professional evaluation, not a self-diagnosis from a forum.
If your concern is purely aesthetic and your face, bite, and airway are functionally normal, a maxillofacial surgeon will usually tell you so. Good surgeons are willing to say no. That honesty is itself a diagnostic test — a practice that will operate on anyone who asks is not the practice you want.
The Bottom Line
Looksmaxxing is just the newest version of something people have always cared about: how their faces look. What’s different now is the amplification—AI filters, crisp 4K video, and social platforms that push transformation content because it performs.
A lot of what gets shared is pretty benign. Some of it actually points people toward real care they might’ve been putting off. And some of it is genuinely harmful.
For maxillofacial surgeons, the trend is a clinical reality that’s not going away. A growing proportion of inquiries now come from young people who learned about jaw surgery through TikTok. A meaningful percentage of them turn out to have real structural issues that warrant evaluation — retruded mandibles, narrow airways, undiagnosed sleep apnea, or skeletal asymmetry. Another meaningful percentage do not, and they deserve a respectful, honest conversation that redirects them toward care appropriate to what’s actually happening with their face.
Dr. Larry M. Wolford and his Dallas practice have spent decades at the intersection of corrective jaw surgery, TMJ disease, and airway medicine — performing more orthognathic revision surgeries than any other maxillofacial surgeon worldwide. For patients who suspect they may have genuine structural jaw issues beyond what a social media trend can diagnose, a free 15-minute telephone consultation at 214.828.9115 is an appropriate first step. Prospective patients can also start with a self-assessment questionnaire or the airway evaluation questionnaire for sleep apnea before scheduling a full consultation.
The face has meaning. It shapes how we communicate, how we’re perceived, and how we experience ourselves in the world. That’s exactly why decisions about modifying it deserve more than a trending hashtag can provide.
Further Reading on drlarrywolford.com
- Meet Dr. Larry M. Wolford
- Orthognathic (Corrective Jaw) Surgery
- Complex Orthognathic Revision Surgery
- Mandibular Condylar Hyperplasia
- Virtual Surgical Treatment Planning
- Airway Evaluation for TMJ and Orthognathic Surgery
- Obstructive Sleep Apnea Corrective Surgery
- Before & After Surgery Results
- Patient Testimonials
- Contact the Office