A couple of years ago, Ozempic was a diabetes drug most people hadn’t heard of. Now it’s in magazine headlines, late-night monologues, and half the conversations happening at your cousin’s wedding. Wegovy, Zepbound, and Mounjaro have joined the club. GLP-1 medications have become one of the biggest health stories of the decade — and they’re quietly changing things in corners of medicine most people never think about.
One of those corners is jaw surgery.
If you’re on a GLP-1 medication, have been on one, or are thinking about starting — and you also deal with jaw pain, a bad bite, snoring, sleep apnea, or you’ve got a maxillofacial procedure on the horizon — there are some things worth knowing that the “Ozempic face” headlines have mostly glossed over. This piece walks through what the research actually says, what’s happening in the operating room, and what patients should be thinking about before, during, and after GLP-1 therapy.
Let’s Start With the Short Version
When people lose weight fast on a GLP-1, the face changes. That part’s real. You’ve probably seen it: hollowed-out cheeks, sunken temples, a sharper jawline, looser skin along the jowls and neck. For most folks it’s a cosmetic issue and nothing more.
But for a smaller group, the changes intersect with what’s going on underneath — jaw anatomy, airway anatomy, TMJ anatomy — in ways that actually matter. Sometimes in a good way. Sometimes not.
At the same time, GLP-1 drugs have turned into a real tool for treating obstructive sleep apnea in obese patients. A phase 3 trial published in 2024 showed tirzepatide cut AHI scores substantially and improved weight, blood pressure, and systemic inflammation. The drugs aren’t replacing CPAP or jaw surgery for sleep apnea, but they’re showing up more and more as part of the plan.
Here’s the thing most people miss: the cosmetic story and the airway story are really the same story. Both are about what happens when you pull a lot of fat off the face and out of the throat in a relatively short window of time.
So What Do These Drugs Actually Do to the Face?
The mechanism isn’t complicated. GLP-1 medications cut your appetite, slow down how fast your stomach empties, and help your body manage blood sugar. In people with obesity, that adds up to serious, sustained weight loss — around 15% of body weight on average with semaglutide, and up to 17% with tirzepatide.
Here’s where it gets tricky, though. The weight doesn’t come off evenly, and it isn’t all fat. Somewhere between a quarter and 40% of what you lose on these drugs is lean muscle. That matters for the face because your face isn’t just skin — it’s a scaffold of fat pads and small muscles holding everything in place. When fat and muscle drop at the same time, faster than the skin can catch up, you get the whole “Ozempic face” look:
- Flattened cheekbones
- Hollowed temples and under-eye areas
- Deeper tear troughs and laugh lines
- Thinner lips
- Looser skin along the jaw and jowls
- A more visible, sharper jawline — which, depending on what your face looked like before, either looks great or looks gaunt
A 2026 systematic review published through Oxford found something striking: in a blinded pilot study, people with massive weight loss were judged to look an average of 5.1 years older than their actual age. Most practicing surgeons would tell you that tracks with what they’re seeing.
Speed is everything here. Lose weight gradually and your skin has time to retract, your tissues have time to redistribute, and your face figures it out. Lose it in six to twelve months — which is pretty typical for GLP-1 therapy — and it doesn’t.
Why Any of This Matters for Jaw Surgery Patients
A few practical things to know if you’re thinking about jaw, TMJ, or airway surgery while you’re on one of these medications.
Your bones are more visible now than they used to be. When someone drops 40 or 60 pounds, the jaw underneath starts showing itself in ways it never did before. Asymmetries, recessions, subtle structural issues — they all get louder when the soft tissue padding goes away. A lot of patients wind up in a maxillofacial consult for the first time in their adult lives after a year on a GLP-1, and they’re not imagining things. The jaw they’ve always had is just finally visible.
For orthognathic surgical evaluation, this is actually useful. The diagnostic picture is clearer. X-rays, 3D imaging, and airway analysis can pick up recessed mandibles, narrow arches, condylar asymmetries, and airway problems that were always there but were hiding under soft tissue. If you’ve got a real underlying skeletal issue — especially combined with sleep apnea or TMJ trouble — this new clarity is an opportunity, not a problem.
Timing matters. A lot. Plastic surgeons have landed on a pretty consistent rule: wait until you’ve been at a stable weight for at least 6 months before elective facial surgery. Peak weight loss on GLP-1 medications usually hits around the one-year mark, so this means most patients need to think in terms of 18 months or so from starting therapy to being ready for cosmetic facial work. The same logic applies to jaw surgery. Operating on someone in the middle of active weight loss, when the face is still changing, makes it harder to predict how things will look once the dust settles.
If what you need is elective — a jaw advancement for mild cosmetic and functional reasons — finish the weight loss first, let things stabilize, and then come in for a fresh evaluation. If it’s urgent — progressive condylar resorption, severe sleep apnea, an ankylosed joint, something actively getting worse — the conversation is different and has to be individualized.
Tell your anesthesiologist. Every single time. This one is non-negotiable. GLP-1 drugs slow down how your stomach empties, which means even after the standard “nothing to eat or drink after midnight” routine, you may still have food in there. That’s an aspiration risk under general anesthesia. The current recommendation is to stop GLP-1 medications several days before surgery and make sure your anesthesiologist knows. Doesn’t matter whether you’re on it for diabetes, weight loss, or off-label — they need to know.
Your bones need protein to heal. This isn’t really about GLP-1s themselves — it’s about what often goes with them. Rapid weight loss sometimes comes with underwhelming protein intake, thin micronutrient reserves, and mild malnutrition that nobody flags because you’re losing weight and technically getting healthier. But jaw surgery requires bone to heal, and bone healing needs building blocks. Most surgeons want to see 20-30 grams of protein per meal, or roughly 1 to 1.5 grams per kilogram of body weight per day, especially in the weeks before and after surgery.
What happens if you stop the medication? The evidence is pretty clear on this: a lot of patients regain weight when they come off GLP-1 therapy. The semaglutide STEP 4 withdrawal trial showed significant regain in people who stopped. For a surgery where the aesthetic outcome depends on a stable facial envelope — a chin procedure, a maxillomandibular advancement, a TMJ reconstruction — future weight changes can shift how things look down the road. It doesn’t undo the functional part of the correction. But the face you see a year after surgery isn’t guaranteed to be the face you have at year five if your weight changes a lot.
The Sleep Apnea Story: This One’s a Real Shift
The most interesting thing happening at the intersection of GLP-1s and maxillofacial surgery is on the airway side.
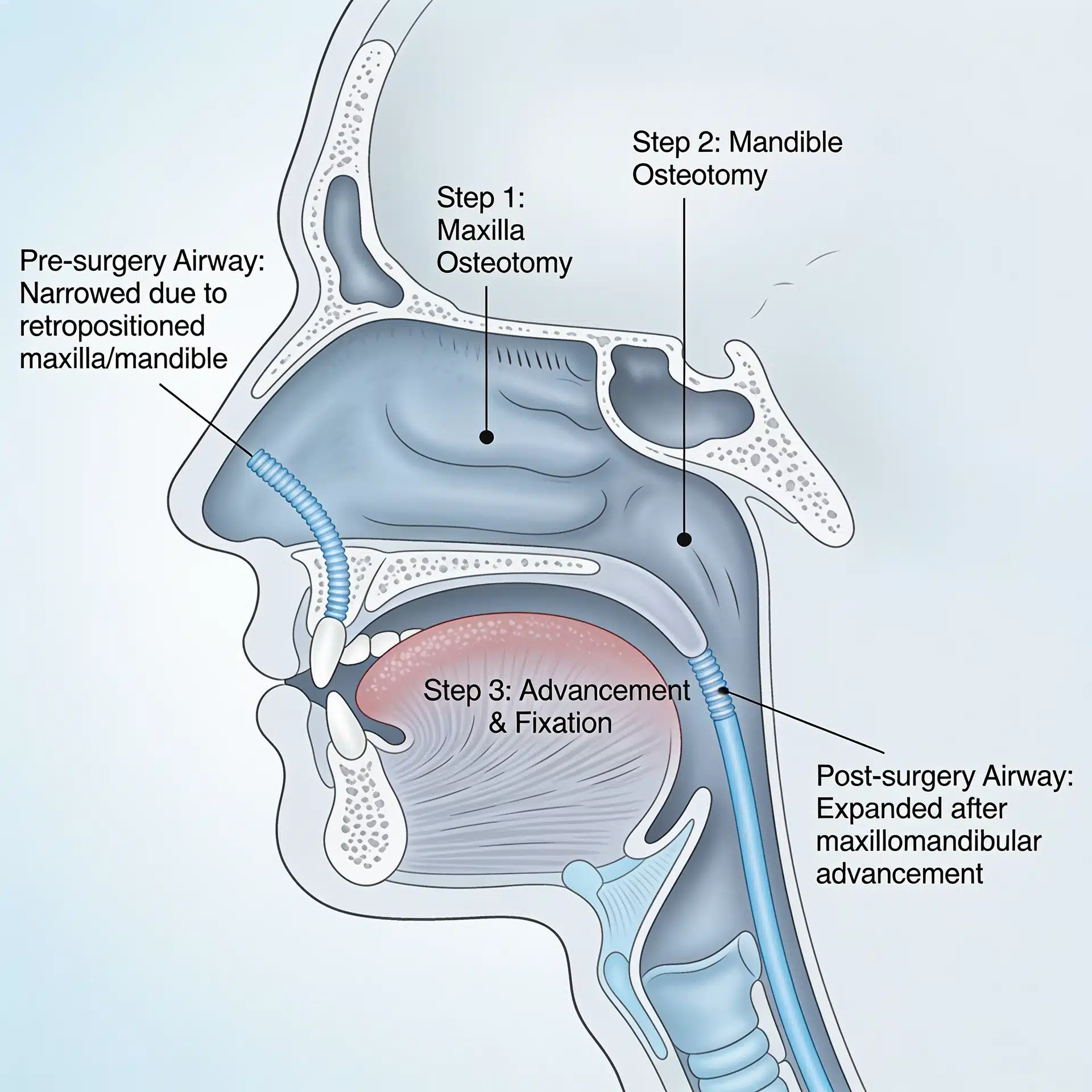
Sleep apnea has always been managed with CPAP, oral appliances, and — for patients who can’t tolerate those or aren’t getting enough benefit — surgery. Maxillomandibular advancement has the best track record of any surgical option, with AHI reductions averaging more than 40 events per hour in the right candidates.
GLP-1 medications have now shown up as a legitimate addition to the toolkit for obese patients. The 2024 tirzepatide trial showed real reductions in AHI, weight, and blood pressure, with bigger benefits in patients with severe obesity and severe OSA. A meta-analysis of six studies covering over 1,000 patients found a pooled AHI reduction of about 9.5 events per hour.
That’s meaningful. But let’s keep it in perspective — 9 or 10 events per hour is a real improvement, but for someone with moderate-to-severe sleep apnea, it usually isn’t going to take them from “sick” to “cured.” Surgery produces AHI reductions four times that size in the right patients. GLP-1 therapy is an adjunct or a stepping stone, not a replacement when your airway anatomy is the problem.
Where GLP-1s are really finding a role in the surgical world is before the OR. A 2025 Laryngoscope review described GLP-1s as a valuable tool for optimizing surgical patients — bringing BMI down, reducing airway fat deposition, and improving surgical candidacy. If you’ve got severe obesity and severe OSA and you’re not an ideal MMA candidate right now, a course of GLP-1 therapy followed by surgical evaluation is a reasonable path.
So who still needs surgery after all this? People whose OSA is really driven by their skeletal anatomy. If you’ve got a recessed jaw, a narrow airway, a craniofacial issue, or a small posterior airway space, weight loss will help — but it won’t move your bones. The fat comes off. The skeleton doesn’t change. For those patients, corrective jaw surgery for sleep apnea is still the answer. Dr. Wolford’s published research, including work on double orthognathic surgery effects on OSA and airway space changes after orthognathic surgery, documents airway corrections that weight loss simply can’t duplicate.
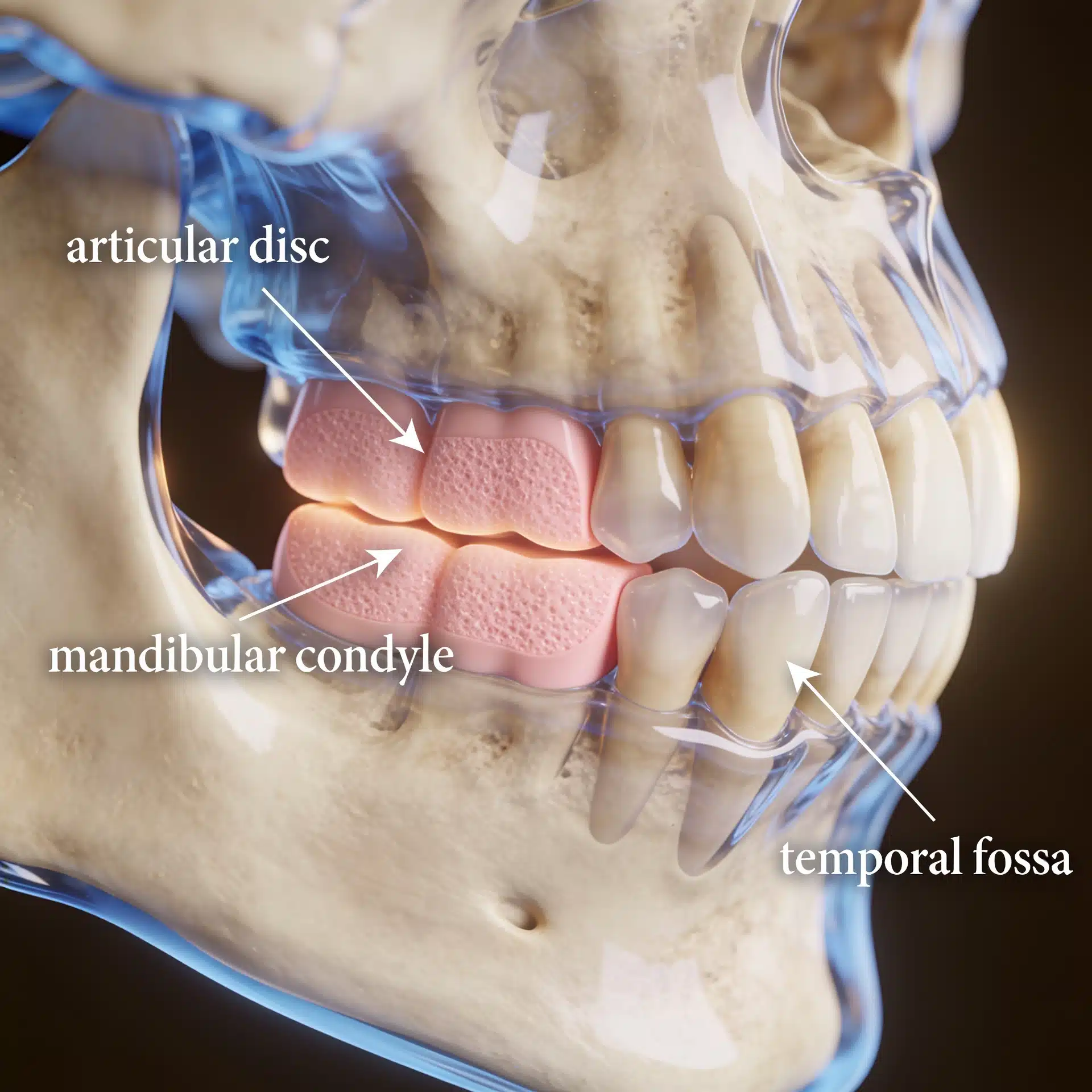
What About TMJ?
This part hasn’t gotten much attention in the mainstream coverage, but it’s worth mentioning.
Some patients with long-standing TMJ symptoms — especially the muscular, soft-tissue kind rather than the structural joint kind — report feeling better after significant weight loss. Inflammation drops, muscle tension patterns can shift, sleep improves (especially if undiagnosed sleep-disordered breathing was contributing). It’s not a reliable effect, but it does happen.
Here’s the more important point, though. If you’ve got structural TMJ disease — condylar resorption, ankylosis, reactive arthritis, or autoimmune-driven joint disease — weight loss is not going to fix it. A resorbing condyle doesn’t regenerate because your BMI dropped.
The real risk here is that big improvements in overall health and appearance can distract from a progressive joint disease that’s quietly getting worse in the background. If you’re on a GLP-1, feeling better in most ways, but your jaw still hurts or clicks or locks, that deserves a proper TMJ evaluation including MRI. Don’t assume the medication is going to eventually take care of it.
A Simple Checklist
If you’re on a GLP-1 or thinking about one, and any of the following apply, it’s worth having a real conversation with both your prescribing doctor and a maxillofacial surgeon:
- You have sleep apnea, or you probably do and haven’t been tested
- You know or suspect you’ve got a jaw deformity, bad bite, or facial asymmetry
- You have ongoing TMJ pain, clicking, locking, or limited opening
- You’ve had jaw surgery before and the results weren’t complete
- You’ve got an elective jaw, cosmetic, or facial procedure on the calendar
- Your face or your bite has changed noticeably since you started losing weight
Good questions to bring with you:
- Am I at a stable weight, or am I still losing?
- Is my airway problem structural or is it going to respond to weight loss?
- If I need surgery, when’s the right time relative to my GLP-1?
- What does my anesthesia plan need to account for?
- Am I getting enough protein to heal well?
- What happens if I go off the medication eventually?
If you’ve got real questions about your jaw, airway, or TMJ and you want to talk to someone, Dr. Wolford’s Dallas office offers a free 15-minute phone consultation at 214.828.9115. You can also start with the TMJ Pain Questionnaire or the Airway Questionnaire for Sleep Apnea on the site — both are useful starting points.
The Bottom Line
GLP-1 medications are doing real good for millions of people. Meaningful weight loss, better blood sugar, lower cardiovascular risk, measurable improvement in sleep apnea for a lot of patients. Those are genuinely important wins.
But they’re also changing the face, the airway, and the visibility of underlying anatomy in ways that jaw surgeons are seeing in clinic every week. For some patients, those changes are cosmetic and nothing more. For others, they bring long-hidden structural issues into view for the first time.
The message for most people isn’t to be afraid of these medications. It’s to integrate them into a bigger plan. GLP-1 therapy is a powerful tool when it’s indicated. It works best when it’s coordinated with a clear understanding of what it can do — weight, metabolism, airway fat — and what it can’t — skeletal correction, structural joint repair, real airway reconstruction.
The worst outcome is when weight loss gets treated as the solution to a problem that’s actually anatomic. The best outcome is getting the diagnosis right — metabolic, airway, jaw, joint — and building a plan that handles each part on its own terms.
Related Reading on drlarrywolford.com
- Meet Dr. Larry M. Wolford
- Orthognathic (Corrective Jaw) Surgery
- Obstructive Sleep Apnea Corrective Surgery
- Airway Evaluation for TMJ and Orthognathic Surgery
- TMJ Dysfunction Overview
- Total TMJ Replacement
- Virtual Surgical Treatment Planning
- Research Publications by Dr. Wolford
- Double Orthognathic Surgery Effects on OSA
- Contact the Office