For a long time, orthognathic surgery was thought of as something you did as a teenager. You finished growing, you wore braces for a few years, and if your bite or jaw alignment needed a surgical correction, you got it done around age 18. If you missed that window — because your family couldn’t afford it, because your orthodontist didn’t flag it, because you were told you’d “grow out of it,” or because you just decided to live with it — the assumption was that ship had sailed.
That assumption is wrong, and the data is finally catching up.
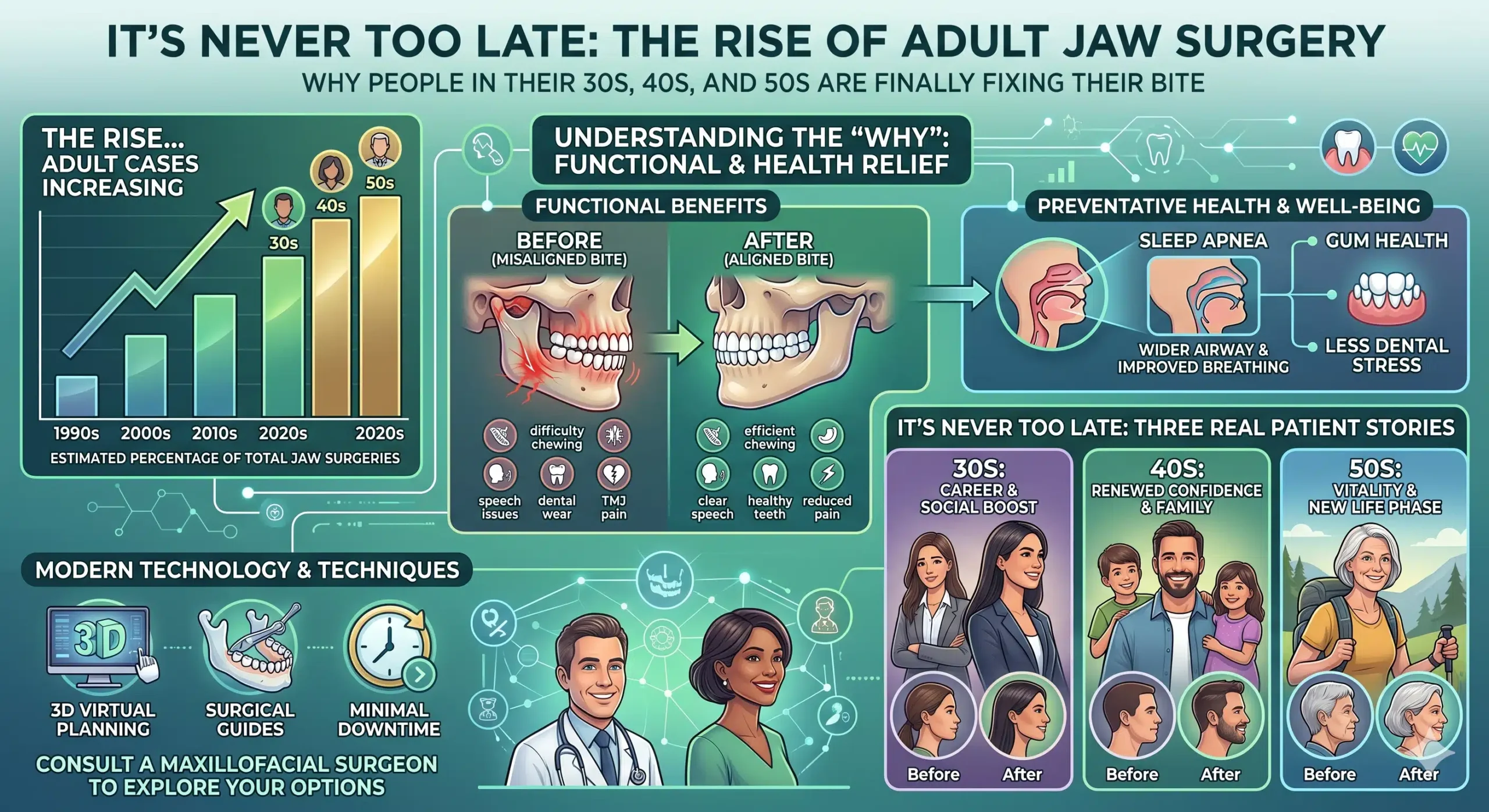
A 2025 nationwide study in Germany looking at nearly two decades of orthognathic surgery data found a 61.8% increase in jaw surgery procedures between 2005 and 2022 — with the biggest jumps happening in the 35-to-59-year-old group (up nearly 67%) and the 60-to-79-year-old group. This isn’t teenagers. It’s adults in the middle and second half of life finally doing something about jaw problems they’ve lived with for decades.
If you’re one of them — if you’ve been carrying around a bite that’s never felt right, a jaw that’s given you trouble since middle school, headaches you’ve learned to ignore, a TMJ that started clicking in college and is now grinding, or a sleep apnea diagnosis that came out of nowhere at 45 — this piece is for you. Because the truth is, corrective jaw surgery works just as well in your 40s as it does in your 20s, and for a lot of adults, it’s the thing that finally fixes something that’s been quietly making their life harder for years.
Why So Many Adults Are Having Jaw Surgery Now
A few things are happening at once to drive this trend.
The problems didn’t go away. They just got louder. Kids with skeletal malocclusions who never got surgical correction grow into adults with the same underlying anatomy — plus years of accumulated wear on their teeth, their jaw joints, and their airway. What was tolerable at 20 often isn’t tolerable at 45. Tooth wear from an abnormal bite becomes expensive dental work. TMJ symptoms that used to come and go become constant. A mild snore becomes obstructive sleep apnea. Problems that were manageable become the thing keeping you up at night — sometimes literally.
Sleep apnea has become a much more common entry point. A huge percentage of adult orthognathic patients in 2026 are showing up because of their airway, not their bite. A CPAP machine that nobody can tolerate. An oral appliance that only half works. A cardiologist telling them their untreated sleep apnea is putting their heart at risk. When a sleep physician suggests a surgical opinion, they end up in a maxillofacial consult — and for the first time, someone looks at their jaw anatomy and says, “You know, the reason your airway collapses at night is that your lower jaw has been recessed since you were 14.” Orthognathic surgery for obstructive sleep apnea has become one of the biggest drivers of the adult jaw surgery boom.
Orthodontics alone, in adulthood, often isn’t enough. Plenty of adults try to fix their bite with Invisalign or braces, only to find that moving teeth around can only do so much when the underlying jaws are misaligned. Teeth can compensate to a point. But if the bones are in the wrong place, no amount of tooth movement produces a stable, functional, healthy bite. A lot of patients only discover this after they’ve already invested a couple of years in adult orthodontics and aren’t seeing the results they hoped for.
The surgery itself has gotten better. Twenty years ago, jaw surgery meant being wired shut for weeks, a long hospital stay, and a recovery that was legitimately brutal. Today’s patients are typically home the same day or the next day, eating soft food within hours, not wired shut at all (rigid fixation with titanium plates has replaced jaw wiring), and back to work within a few weeks. Computer-assisted surgical planning, patient-specific fixation, and a better understanding of airway dynamics have dramatically improved outcomes and reduced morbidity compared to the old days. The procedure isn’t what your uncle had in 1985.
Awareness is finally catching up. People understand now that jaw misalignment isn’t just cosmetic. It’s functional. It affects chewing, speaking, breathing, sleeping, and — over time — your TMJs and your teeth. As that understanding spreads, more adults are looking at their own situation and asking whether something they’ve put up with forever is actually fixable.
Is There a Maximum Age?
Short answer: no.
Current clinical guidance is clear that there’s no upper age limit for orthognathic surgery as long as the adult patient is in good overall health. Plenty of patients in their 50s, 60s, and even 70s undergo successful jaw surgery every year. What matters is medical fitness, not chronologic age.
The research on older orthognathic patients is actually pretty reassuring. A multi-institutional study looking at patients over 40 found that older patients have somewhat longer hospital stays and slightly higher rates of hardware removal down the line, but that the core outcomes — stable bite correction, functional improvement, quality of life gains — are excellent. And because jaw growth is completely finished in adults, the long-term stability of the surgical result is typically better in older patients than in teenagers. There’s no residual growth to undo your correction.
The bigger-picture research is even more encouraging. A 2025 retrospective review of orthognathic surgery outcomes documented significant improvements in quality of life, self-esteem, body image, and emotional stability after surgery — in an adult patient population. The psychological benefits of finally having a functional, stable bite aren’t just marketing. They’re measurable.
What Adults Are Actually Coming In For
The profile of an adult orthognathic patient is genuinely different from a teenage one. Teenagers are usually there because their orthodontist told their parents surgery was needed to finish the bite correction. Adults almost always have a story.
A few of the most common ones:
“My bite has been getting worse.” This is sometimes progressive condylar resorption, particularly in women in their 20s and 30s — a condition where the jaw joint bone is actively being lost, and the bite is shifting because of it. It’s often missed for years and misdiagnosed as “just TMJ.” By the time it’s accurately identified, there’s usually both structural joint disease and a progressive malocclusion that need to be corrected together.
“I’ve had jaw surgery before and it didn’t hold.” Complex orthognathic revision surgery is one of the hardest areas of maxillofacial medicine, and it’s exactly the area where Dr. Wolford’s practice is known worldwide. Patients who had a single-jaw surgery years ago — often without the TMJ being properly evaluated — and have since developed pain, relapse, or an unstable bite are a large and growing group. The good news is that revision is entirely possible. It just requires a surgeon who does this kind of work all the time.
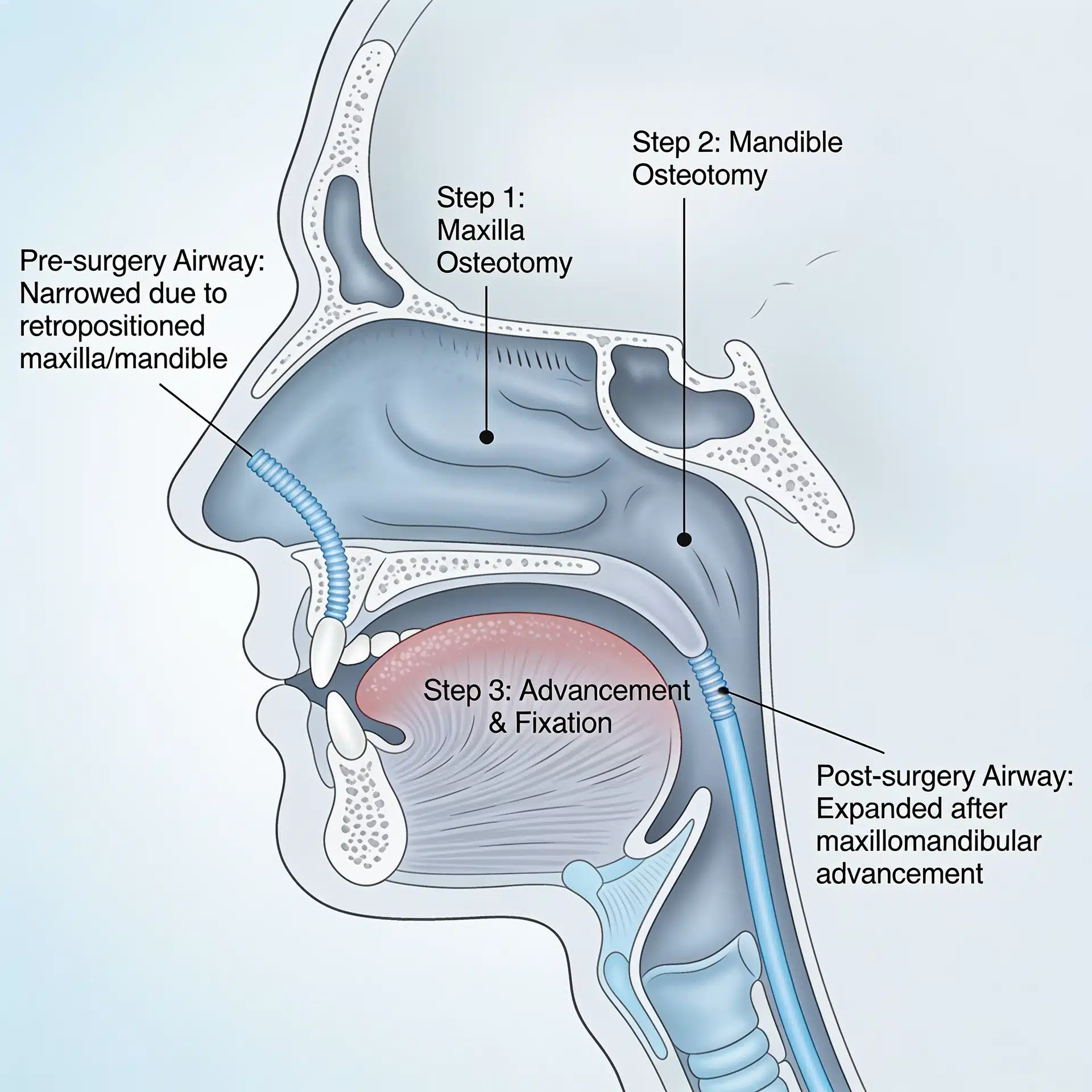
“My sleep apnea is serious and CPAP isn’t working.” For adults with retruded lower jaws and airway-driven obstructive sleep apnea, maxillomandibular advancement is often the most effective long-term solution available. AHI reductions from MMA average much larger than what weight loss, oral appliances, or even GLP-1 medications can deliver, because the procedure physically enlarges the airway in three dimensions.
“My face has always looked asymmetric.” Mandibular condylar hyperplasia — a growth disorder that causes one side of the jaw to overgrow or grow unevenly — can go undiagnosed for years. Patients learn to tilt their head in photos. They never really look at themselves straight on. As adults, many finally want to address it — and modern surgical planning can achieve a level of correction that wasn’t possible a generation ago.
“I have constant jaw pain and headaches.” When TMJ dysfunction is driven by an underlying skeletal jaw problem, addressing the jaw is often the only way to actually resolve the symptoms. Patients who’ve cycled through splints, physical therapy, injections, and medications for years sometimes discover that their joint is suffering because of where their bones are — and fixing the bones fixes the joint.
“My teeth are falling apart from years of wearing them unevenly.” Patients with long-standing malocclusions often end up with severely worn teeth, repeatedly broken crowns, or advanced TMJ arthritis by their 40s. When a restorative dentist looks at a mouth like that, they know that placing more crowns on a bad bite is a temporary fix. The bite itself needs correcting first.
What the Process Actually Looks Like for an Adult
One thing that surprises adult patients is how different the modern orthognathic workflow is from what they might have imagined.
A comprehensive evaluation comes first. This typically includes a full dentofacial deformity evaluation, three-dimensional imaging (CBCT or CT scan), MRI evaluation of the TMJs when joint involvement is suspected, an airway assessment, and a careful review of the patient’s full history — medical, dental, orthodontic, and symptomatic. Adults often have complex histories that matter. A surgery plan built on incomplete information is a surgery plan that fails.
Pre-surgical orthodontics is usually part of the picture — but not always. Traditionally, patients spent 12 to 18 months in pre-surgical orthodontics to prepare the teeth for their new post-operative position. That’s still the most common path. But “surgery-first” approaches have become more common in certain cases, where the bones are repositioned first and the teeth are aligned around the new skeletal foundation. For adults who don’t want to spend two years in braces before their surgery, this can be an option worth discussing.
Virtual surgical planning is now standard for complex cases. The surgeon walks the patient through a 3D simulation of exactly what’s going to happen — which bones move, how far, in which direction, and what the predicted result looks like. For adults who are nervous about committing, this kind of visual transparency is often the thing that tips them from “thinking about it” to “doing it.”
The surgery itself is typically a single procedure — or a coordinated set of procedures. A double-jaw surgery (both upper and lower jaws repositioned in the same operation), often combined with a chin procedure (genioplasty) and, when indicated, simultaneous TMJ work, is done in one trip to the OR. Most patients stay one night in the hospital.
Recovery is demanding but not the nightmare it used to be. The first week or two involves significant swelling, a soft-to-liquid diet, and careful wound care. Most adults are back to sedentary work in 2-4 weeks and fully recovered at 3-6 months. Nerve sensation recovery (particularly to the lower lip and chin) can take longer and is one of the specific things to discuss thoroughly with your surgeon before proceeding.
The functional improvement is usually the part patients talk about the most. Patients often report that the aesthetic change was nice but the functional change was life-altering. Being able to chew properly. Being able to close your mouth without strain. Sleeping through the night for the first time in years. Headaches that had been part of life for two decades just… stopping.
What Adults Should Think About Before Deciding
A few things that matter more at 45 than they did at 18.
Your overall medical picture. Controlled hypertension, diabetes, autoimmune disease, cardiac history, medications — all of this needs to be fully disclosed and factored in. Most adults are perfectly reasonable surgical candidates, but the pre-operative workup is more thorough.
Bone density. Post-menopausal women and older patients sometimes benefit from a baseline bone density check and optimization of vitamin D and calcium before surgery. Bone healing is one of the most important factors in orthognathic recovery.
Time and logistics. Adults have jobs, families, and responsibilities that teenagers don’t. Planning a 2-4 week recovery window, arranging help at home, and thinking through how the first few weeks will actually work is part of preparing for the surgery, not an afterthought.
Realistic expectations. Modern orthognathic surgery delivers dramatic, durable improvements. It doesn’t make you 25 again, and it doesn’t produce the filtered-photo face of a TikTok before-and-after. A good surgeon will walk you through exactly what to expect and won’t promise more. If a practice is promising miracles, that’s a reason to be skeptical, not reassured.
The surgeon matters more than anything else. This is the single most important variable in the entire process. Revision jaw surgery, complex TMJ-orthognathic cases, and older adults with medical complexity are not cases for a low-volume practice. Dr. Wolford has performed more orthognathic revision surgeries than any other maxillofacial surgeon in the world — which matters precisely because adult orthognathic patients are disproportionately the ones who need revision or concomitant TMJ work.
The Bottom Line
The old rule that said jaw surgery was a teenage procedure is dead. Adults make up the fastest-growing segment of orthognathic surgery patients worldwide, and for good reasons — the problems were always there, they just finally got serious enough (or loud enough, or painful enough) to fix. Functional outcomes in adults are excellent. Stability is excellent. Quality-of-life improvements are genuinely striking. And the surgery itself is dramatically easier to go through than it was a generation ago.
If you’ve been living with a jaw problem for years or decades — a bad bite, chronic TMJ pain, untreated sleep apnea, facial asymmetry, failed prior orthodontics or surgery — the fact that you’re 35 or 50 or 65 is not the barrier you may have assumed it was. What matters is whether the underlying problem is real, whether you’re healthy enough for surgery, and whether you have a surgeon with the experience to do it right.
It’s almost never too late to fix a jaw. For a lot of adults, it turns out to be the single best health decision they make.
Dr. Wolford’s Dallas office offers a free 15-minute phone consultation at 214.828.9115 for adults who want to explore whether their situation is a candidate for surgical evaluation. The TMJ Pain Questionnaire and the Airway Questionnaire for Sleep Apnea are useful starting points before a full consultation, and patients traveling from outside Texas can find practical information on the Travel Information page.
Related Reading on drlarrywolford.com
- Meet Dr. Larry M. Wolford
- Orthognathic (Corrective Jaw) Surgery
- Complex Orthognathic Revision Surgery
- Orthognathic Surgery Evaluation
- Virtual Surgical Treatment Planning
- TMJ Dysfunction Overview
- Total TMJ Replacement
- Mandibular Condylar Hyperplasia
- Obstructive Sleep Apnea Corrective Surgery
- Before & After Surgery Results
- Patient Testimonials
- Contact the Office