Here’s a scenario that plays out more often than it should.
A teenage girl — 14, 15, maybe 16 — starts complaining about jaw pain. Her bite feels different. Her chin looks like it’s getting smaller, or pulling back. Her front teeth don’t meet the way they used to. Her parents take her to the orthodontist, who thinks it’s a typical Class II malocclusion — a common overbite pattern — and starts treatment with braces, possibly with elastics, possibly with headgear.
A year goes by. The bite isn’t improving. It’s getting worse.
Another year goes by. Now there’s an open bite up front — her front teeth can’t touch at all. Her lower jaw has clearly pulled backward. She’s developing headaches. Her TMJs click and pop. Her face is changing shape in photos. The orthodontist is frustrated. The parents are frustrated. The patient is frustrated and, often, starting to feel self-conscious about her face.
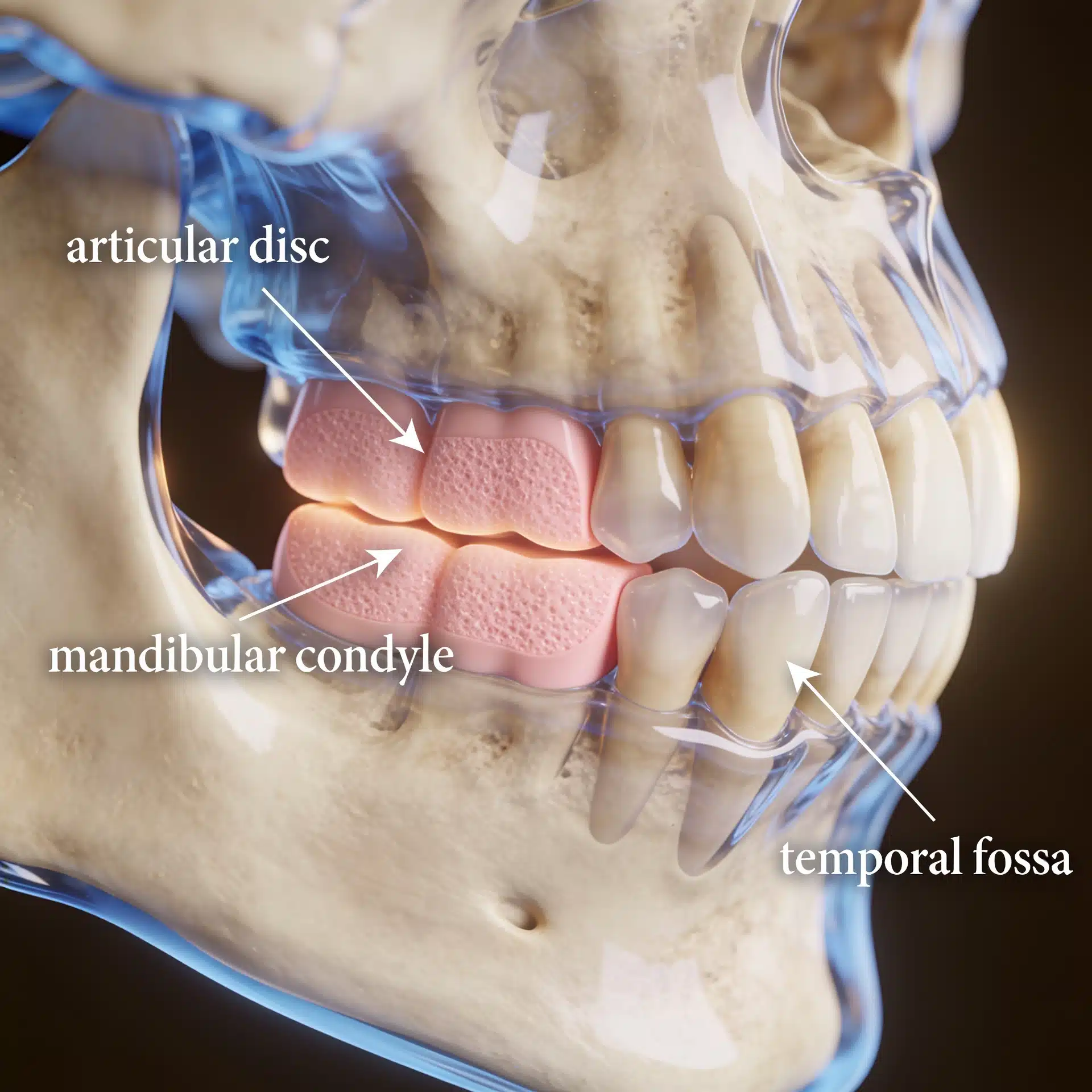
By the time someone finally orders an MRI of the TMJs, the damage is already done. The condyles — the ball-shaped tops of her lower jaw that form the jaw joint — are visibly smaller than they should be. Bone has been lost. The discs are dislocated. What everyone thought was an ordinary orthodontic problem turns out to be something called idiopathic condylar resorption, and it’s been actively destroying her jaw joints the entire time.
This is one of the most heartbreakingly common stories in maxillofacial medicine — and one of the most important to catch early. Because with the right recognition, the right surgeon, and the right treatment plan, the outcome can go from “a face that’s going to keep deteriorating” to “stable, functional, and healthy for the rest of her life.” But the catch has to come early.
If you’re a parent, a young woman, an orthodontist, a pediatrician, or anyone who just stumbled onto this article because something about it sounds uncomfortably familiar — keep reading.
What ICR Actually Is
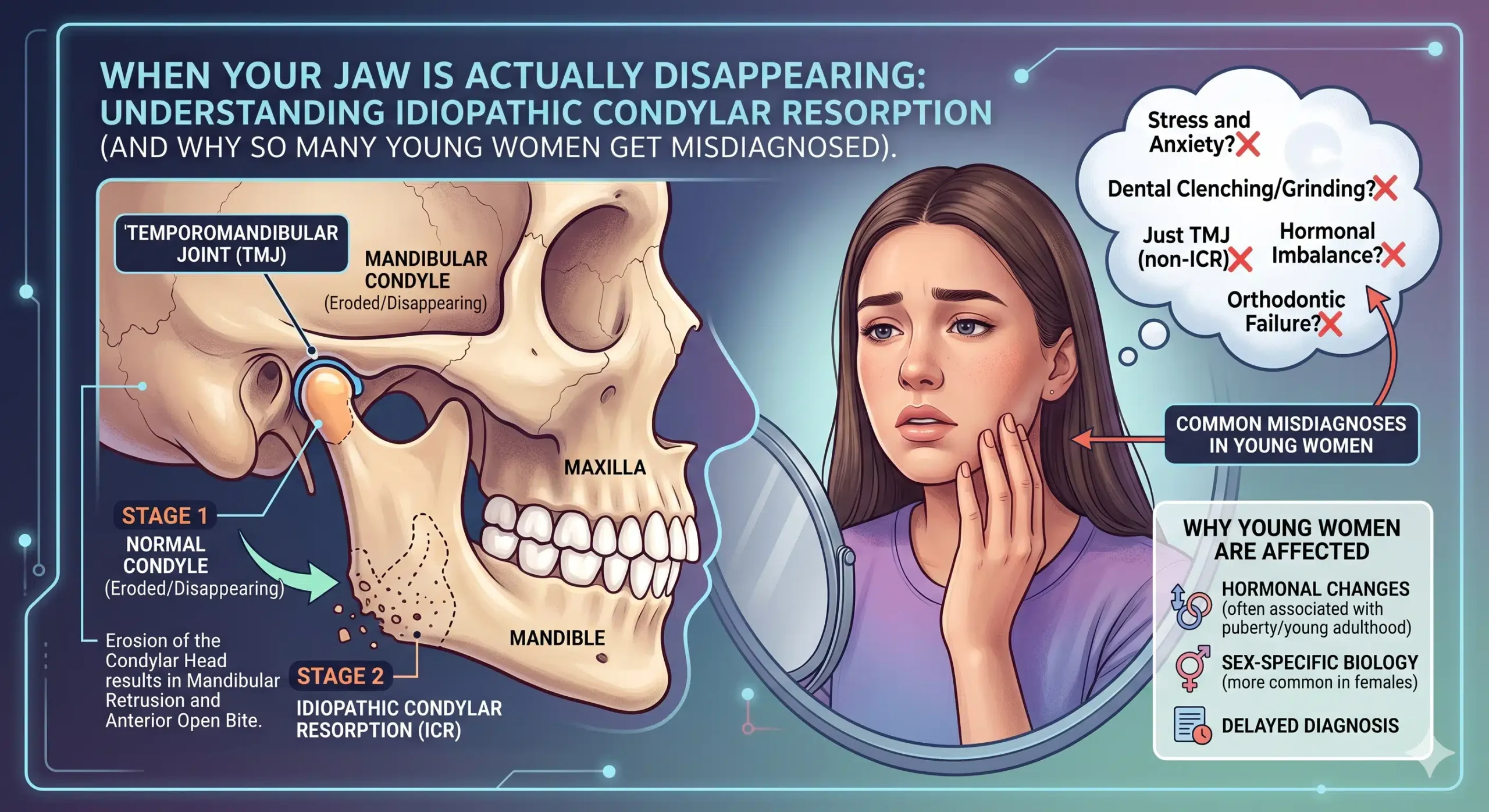
Idiopathic condylar resorption — also called ICR, progressive condylar resorption, adolescent internal condylar resorption (AICR), or, more colloquially, “cheerleader’s syndrome” — is a progressive disease of the temporomandibular joint in which the condylar bone is slowly being destroyed.
“Idiopathic” just means “we don’t fully know what causes it.” “Condylar resorption” means the condyle (the top of your lower jaw, the part that fits into the socket of your skull to form the jaw joint) is being actively resorbed — the body is breaking down bone that should be staying intact.
As the condyle shrinks, a cascade of predictable changes follows: the lower jaw loses vertical height on that side, the mandible rotates backward and downward, the chin retrudes (pulls back), and the bite opens at the front. If it’s happening on both sides — which it often is — you get a symmetric version of all of that, leading to the classic presentation: a progressively retruding lower jaw, a Class II bite, an anterior open bite, and often TMJ pain or dysfunction.
The condition overwhelmingly affects young women, with a female-to-male ratio somewhere between 9:1 and 16:1. It most commonly shows up in teenage girls during or shortly after the pubertal growth spurt, typically between ages 11 and 45, with the peak window being roughly 15-35. Orthodontists estimate they see about 1 case of ICR for every 5,000 orthodontic patients — which sounds rare, but when you add up every orthodontic practice in the country, it’s a lot of young women being affected.
The “cheerleader’s syndrome” nickname comes from the observation that many patients are thin young women involved in sports, and that minor or major jaw trauma — the kind that can happen with gymnastics, dance, cheerleading, soccer, or any athletic activity — can initiate or worsen the process. It’s not a great name (the disease isn’t caused by being a cheerleader), but it’s stuck around because it captures the demographic pattern well.
Why It Happens — What We Think We Know
This is where things get genuinely uncertain, and honest doctors will say so. The cause of idiopathic condylar resorption isn’t fully understood, but several theories have accumulated decent evidence over the last few decades.
The hormonal theory. The dramatic female predominance has pushed researchers toward estrogen as a central player. The temporomandibular joint contains estrogen receptors (specifically ERβ), and some research has suggested that low estradiol levels — including the low-estrogen states that can occur in young athletic women with irregular cycles — may be associated with increased risk. This is part of why the disease clusters around puberty and why it rarely appears in post-menopausal women (the hormone disruption window is different).
The avascular necrosis theory. The idea here is that the blood supply to the condyle gets compromised — by microtrauma, by mechanical overload, by vascular issues — and bone begins to die from inadequate perfusion. In patients with a very specific skeletal profile (high mandibular plane angle, Class II skeletal pattern, retruded mandible), the mechanical loads on the condyle may be abnormal enough to push the vascular supply past its breaking point.
The dysfunctional remodeling theory. Bone is constantly being broken down and rebuilt throughout life — a process called remodeling. In ICR, something tips the balance so that more bone is being resorbed than laid down, and the condyle shrinks over time.
The mechanical loading theory. Patients with certain jaw shapes — high occlusal and mandibular plane angles, Class II skeletal patterns — appear to load their jaw joints in ways that predispose them to resorption. This is part of why the skeletal pattern is so consistent across ICR patients.
The most likely answer is probably “all of the above, interacting.” A young woman with a certain skeletal structure, hormonal profile, and activity pattern hits a perfect storm — and the condyle starts to disappear. Once it starts, without intervention, it tends to keep going.
The Classic Presentation — What to Watch For
ICR doesn’t announce itself with a diagnostic flashing light. It looks, initially, like a lot of other things — which is why it gets missed so often. But there’s a pattern, and once you know the pattern, it becomes much easier to spot.
The person. Almost always a young woman, typically between 11 and 30, often thin and athletic. Sometimes with a history of minor jaw trauma (a fall, a sports injury, a dental procedure with prolonged mouth opening). Sometimes with menstrual irregularities or a history of disordered eating. Sometimes none of those things — just a teenage girl who had a normal jaw until she didn’t.
The face. Early on, subtle changes — a slightly more recessed chin, a face that looks a little longer, a jawline that’s starting to look less defined. Family members often notice before anyone else. Photographs taken six months apart can be strikingly different.
The bite. This is the most important clinical sign. The bite changes over time. Front teeth that used to touch no longer touch. An open bite develops or deepens. The lower jaw feels like it’s pulling back. Patients often describe “my bite doesn’t feel right anymore” or “I can only chew on my back teeth.”
The TMJ symptoms. Clicking, popping, or grinding in the jaw joints. Pain, often worse with chewing or wide opening. Limited opening. Headaches, particularly in the temples. Ear fullness or ringing. These symptoms can come and go.
The orthodontic red flag. A patient in active orthodontic treatment whose bite is worsening despite treatment — or whose “Class II correction” just isn’t holding — deserves imaging to rule out condylar resorption. This is the scenario where ICR gets missed for years: the assumption is that the orthodontics just isn’t working well enough, so more elastics, more headgear, more time is applied. Meanwhile, the underlying disease is making everything worse.
The serial-photograph test. One of the most useful informal diagnostic tools is comparing profile photographs from 6-12 months apart. In ICR, the mandible is progressively retruding — and in photos, you can see it. Parents who suspect something is off often have the data on their phones already.
Why the Diagnosis Is Often Delayed
There are a few reasons ICR gets missed or misdiagnosed, and they’re worth understanding.
It looks like common orthodontic problems. A retruding mandible, a Class II bite, an anterior open bite — these are all common patterns. Most of the time, they’re not caused by active bone loss; they’re just how that person’s face happened to grow. Distinguishing “benign skeletal pattern” from “active pathological resorption” requires imaging that often doesn’t get ordered.
Plain X-rays don’t always show it. Panoramic and cephalometric X-rays can be normal or nearly normal early in the disease. The resorption is often better visualized on cone-beam CT or MRI — studies that are not routinely ordered on every orthodontic patient with a funny bite.
MRI is the gold standard, but it’s not standard. MRI is the single best imaging study for TMJ pathology because it shows the soft tissue — including the articular disc — as well as the bone. An MRI on a patient with ICR typically shows loss of condylar volume (often bilaterally) and anterior displacement of the articular discs. But MRIs are expensive, require specific protocols to show the TMJ properly, and aren’t part of most orthodontic workups.
Orthodontists see it once in thousands of patients. At roughly 1 case in 5,000 orthodontic patients, a general orthodontist can reasonably go years without seeing a confirmed case of ICR. By the time pattern recognition kicks in, damage has often accumulated.
Symptoms get attributed to anxiety or growing pains. Jaw clicking, headaches, and bite changes in a teenage girl get written off more often than they should. Sometimes by well-meaning clinicians, sometimes by the patient herself trying to be a good sport about it.
The disease is sometimes treated with the wrong orthodontics. Some literature has warned that aggressive orthodontic treatment of what looks like a simple Class II malocclusion can actually exacerbate condylar resorption when ICR is the underlying problem. The wrong treatment doesn’t just waste time — it can make things worse.
What to Do If You Suspect ICR
The single most important thing — for patients, parents, orthodontists, and primary care clinicians — is to get the right imaging and the right specialist involved early.
Imaging. If ICR is suspected, an MRI evaluation of the TMJs, combined with a cone-beam CT or conventional CT of the jaws, provides the anatomic picture needed to make an accurate diagnosis. Serial cephalometric radiographs over time can also document the progression of mandibular retrusion.
Rule out the other causes. Idiopathic condylar resorption is a diagnosis of exclusion — meaning, before you call it “idiopathic,” you have to rule out the other things that cause condylar resorption. Rheumatoid arthritis, psoriatic arthritis, lupus, scleroderma, reactive arthritis, infection, and traumatic injury can all resorb condyles. That’s why a proper workup for ICR includes rheumatologic labs, a careful medical history, and sometimes referral to rheumatology to confirm that no systemic disease is driving the joint destruction. Dr. Wolford’s practice separately addresses TMJ reactive arthritis and connective tissue and autoimmune disease involvement of the TMJ precisely because the treatment approaches differ.
Get to a surgeon who actually treats this. This is not a condition to manage in a practice that sees it once every five years. ICR is one of Dr. Wolford’s published specialties — his work on the adolescent internal condylar resorption protocol has informed how the condition is treated worldwide. For complex cases, getting to a high-volume center matters enormously.
How ICR Is Treated
This is where the story gets more hopeful. ICR is treatable, and with the right approach, the results can be genuinely excellent — especially when the diagnosis is caught early.
Over the decades, several approaches have been proposed and refined. The general categories include:
Joint-preserving surgery. In early or moderate cases — particularly in younger patients where some growth potential may remain — repositioning the articular disc, stabilizing the joint, and performing concomitant orthognathic surgery to correct the bite and jaw position can halt the progression of the disease and restore function. This approach aims to save the patient’s own joint while arresting the resorption. Dr. Wolford’s published work on adolescent internal condylar resorption has specifically documented cases where early surgical treatment allowed a reversal of the disease process and even some return of normal growth in patients treated young enough.
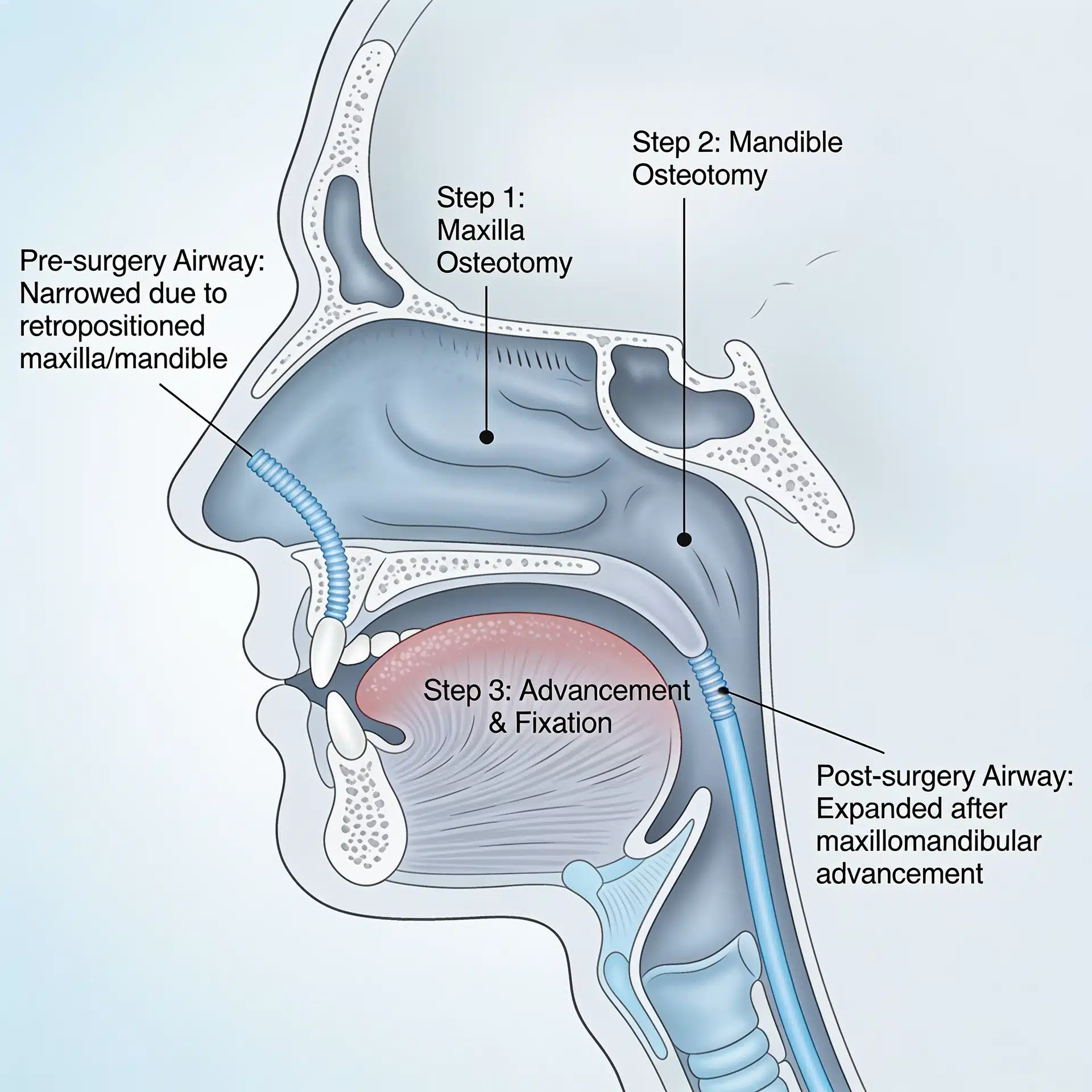
Total TMJ replacement. For more advanced cases, or for patients in whom disc repositioning isn’t sufficient, total TMJ replacement with a patient-specific alloplastic (custom-made) prosthesis is often the definitive answer. Modern prostheses — designed with 3D imaging, virtual planning, and custom manufacturing — can be fit exactly to the patient’s anatomy. When combined with concomitant orthognathic surgery to correct the bite and jaw position, this approach can produce stable, durable, life-changing results. The scoping review literature on modern TMJ reconstruction describes patient-specific alloplastic prostheses as the emerging standard for advanced cases.
Concomitant TMJ and orthognathic surgery. This is the core principle of Dr. Wolford’s approach to ICR and other end-stage TMJ disease: the joint and the jaw have to be treated together, in the same surgery, because they’re one biomechanical system. Fixing the bite without addressing the failing joint leads to relapse. Replacing or repairing the joint without correcting the malocclusion leads to continued dysfunction. Concomitant TMJ and orthognathic surgery solves both problems at the same time.
What about conservative management? For some patients with very early or non-progressive disease, conservative management — soft diet, splint therapy, anti-inflammatory medication, physical therapy — can be appropriate as a first step, particularly while imaging is being repeated to confirm whether the disease is actively progressing or has burned out. But for actively progressing disease, conservative management is buying time, not solving the problem. The longer you wait, the more condylar bone is lost and the harder the eventual reconstruction becomes.
Why Early Treatment Matters So Much
The single most important variable in long-term outcomes for ICR is timing. Dr. Wolford’s published series on adolescent internal condylar resorption has consistently shown that early detection and early surgical management produce the best functional, occlusal, and aesthetic outcomes — with reduced resorption of the condyle, less distortion of the disc, and better long-term loading of the joint structures.
In plain English: the earlier you catch it, the more condyle you have left to save, and the better the final result.
That’s the opposite of the standard course for many ICR patients, which looks like: years of orthodontic treatment that doesn’t work, increasing bite deformity, worsening TMJ symptoms, a face that’s shifting shape month by month, and finally — after all that — a diagnosis and a surgical plan. By then, there’s often much less condyle to work with, and the reconstruction required is more extensive.
This is why the message for parents, young women, and clinicians is urgent: if a teenage or young adult woman’s bite is actively getting worse, if her jaw is visibly retruding, if TMJ symptoms are progressing — get the imaging. Get the specialist opinion. Don’t wait.
For Parents, Specifically
If your daughter is in orthodontic treatment and something feels off — if her bite is getting worse instead of better, if her face is changing shape, if she’s having jaw pain that isn’t improving — you’re allowed to push. You’re allowed to ask whether idiopathic condylar resorption has been considered. You’re allowed to ask for an MRI. You’re allowed to get a second opinion from a maxillofacial surgeon who sees this condition regularly.
Most of the time, your concern will turn out to be ordinary growing pains or orthodontic growing-in. But if it isn’t — if your daughter really is losing condylar bone — catching it six months earlier instead of two years later can be the difference between saving her jaw joints and reconstructing them.
The Bottom Line
Idiopathic condylar resorption is one of the most under-recognized TMJ diseases in medicine. It almost exclusively affects young women. It progresses silently, often hiding behind what looks like a common orthodontic problem. And it responds beautifully to the right treatment — if it’s caught early enough.
The diagnostic challenge is real. The emotional challenge, for families going through it, is enormous. But the outcomes when the condition is correctly identified and properly treated are genuinely excellent. Young women who had active, progressive jaw destruction at 15 can be functionally stable, beautifully aligned, and pain-free at 25 — with the right surgeon, the right plan, and the right timing.
If any of this sounds uncomfortably familiar — a daughter, a friend, a patient, or your own story — it’s worth the phone call. Dr. Wolford’s Dallas office has spent decades building a worldwide reputation specifically in treating condylar resorption, TMJ disease, and concomitant jaw surgery, and offers a free 15-minute phone consultation at 214.828.9115. The TMJ Pain Questionnaire is a useful self-assessment starting point, and patients travel to Dallas for evaluation from cities across the country and around the world.
The jaw you or your daughter is losing is not a jaw that has to keep disappearing. The condition has a name. It has a treatment. And the people who know how to treat it are out there.
Related Reading on drlarrywolford.com
- Meet Dr. Larry M. Wolford
- Mandibular Condylar Resorption
- Adolescent Internal Condylar Resorption (AICR)
- TMJ Reactive Arthritis
- Connective Tissue and Autoimmune Diseases (CT/AI)
- TMJ Trauma
- TMJ Ankylosis
- Total TMJ Replacement
- Complex Orthognathic Revision Surgery
- MRI Evaluation for TMJ
- TMJ Pain Questionnaire
- Before & After Surgery Results
- Contact the Office