If you’ve been living with jaw pain, limited opening, chronic headaches, or that unrelenting click-and-pop every time you chew, 2026 may be the most significant year for TMJ research in a generation. This spring, patient enrollment is ramping up for the TMD IMPACT Initiative — the largest federally funded research effort ever dedicated to temporomandibular disorders. For the millions of Americans managing a diagnosis that has historically been misunderstood, underfunded, and inconsistently treated, that’s genuinely big news.
Along with the headlines comes a flood of marketing: new splints, AI apps, digital therapeutics, regenerative injections, “miracle” conservative protocols. It’s a lot to sort through, especially for patients whose disease has already moved past the point where conservative care can help. How long should you stick with a splint? Does arthrocentesis actually buy you time, or just delay the inevitable? At what point do you stop trying one more thing and go get evaluated for reconstructive surgery? This article unpacks what’s changing in TMJ care this year, what the research actually says, and how patients with advanced disease — condylar resorption, ankylosis, end-stage arthritis, connective tissue disease, or failed prior surgeries — should think about their options.
Why TMJ Care Is Suddenly a National Research Priority
Temporomandibular disorders hit somewhere between 8 and 12 percent of Americans. That makes TMD the second most common musculoskeletal condition in the country, behind only lower back pain. For decades, though, funding for research and agreed-upon ways to diagnose it fell well short of what a problem this widespread should have commanded. The 2020 report on TMD from the National Academies of Sciences, Engineering, and Medicine laid that gap out plainly and pushed for a coordinated federal response.
The National Institute of Dental and Craniofacial Research (NIDCR) has now answered that call. The TMD IMPACT Initiative is structured as a multi-institutional research network spanning universities, clinical sites, and disciplines — a dramatic departure from the isolated single-center studies that dominated the field for decades. The initiative’s goals include detecting biomarkers, standardizing diagnostic criteria, developing customized treatment protocols, and — critically — defining which patients will respond to which interventions.
At the center of this effort is a $17 million CREATE Center grant awarded to the University of Pittsburgh, representing the single largest investment the NIDCR has ever made in TMD research. Parallel NIDCR-supported projects are also exploring:
- TMJ disc tissue engineering using bioactive scaffolds and stem cells to regenerate damaged cartilage
- Biomarker discovery for predicting disease progression
- Non-opioid pain therapeutics, including engineered antibodies that block pain-signaling pathways
- Gut microbiome research connecting systemic inflammation to jaw pain
- Low-level laser therapy trials for conservative pain control
This is the most serious research moment TMJ medicine has ever had. For patients, though, the important takeaway is more immediate: the field is finally being forced to distinguish between TMJ problems that will resolve with conservative care and TMJ problems that will not, no matter how many splints, exercises, or injections you try.
The Conservative Care Question: What the Data Actually Shows
International consensus still holds — and is reinforced by the NIDCR — that reversible, conservative therapies should be the first line of treatment for most patients. Published data suggests that 75% to 90% of patients respond to less invasive management, including physical therapy, diet modification, custom occlusal splints, stress management, and short-term pharmacologic support.
That’s an important number, but it’s also a widely misread one. It does not mean 75–90% of every patient who walks into a TMJ clinic will get better with a nightguard. It means that when the wider TMD population is studied — the bulk of which is myofascial pain, minor disc displacement, and muscle-mediated dysfunction — most patients improve with conservative care. The data says very little about the smaller but profoundly affected subgroup of patients whose TMJs are structurally failing.
This distinction matters because aggressive first-line surgery is genuinely inappropriate for most people. The NIDCR has cautioned patients against irreversible procedures as first-line treatments for a reason: a long history of patients receiving unnecessary orthodontic, occlusal, or surgical procedures that didn’t resolve symptoms — and sometimes made them worse.
But the inverse is equally true. Patients with structural, destructive, or end-stage TMJ pathology are not served by endlessly extending conservative care. For them, the critical question isn’t whether to consider surgery; it’s which surgery, when, and with whom.
The Digital Therapeutics Wave — And Its Limits
At CES in early 2026, a Korean health-tech firm generated major TMJ buzz with the launch of Clickless, an AI-powered digital therapeutic pairing facial movement tracking with cognitive behavioral therapy protocols. South Korea’s Ministry of Food and Drug Safety cleared the device in late 2025, and it’s being marketed as an at-home program that walks TMD patients through structured pain management.
It is not yet FDA-approved in the United States, and it belongs to a growing category — digital therapeutics — that also includes app-based CBT programs, remote physical therapy coaching, and biofeedback tools. For patients with mild to moderate muscle-mediated TMD, these tools may offer meaningful help. They fit a modern care model: low cost, accessible, and sustaining of the biopsychosocial approach the field is moving toward.
But for patients with confirmed internal derangement, condylar resorption, ankylosis, rheumatoid or reactive arthritis, or post-surgical failure, digital therapeutics will not repair damaged anatomy. An app cannot rebuild a resorbed condyle. A CBT protocol cannot reposition a dislocated disc that has been displaced for years. The risk for patients with advanced disease is not that these tools fail — it’s that they delay an appropriate surgical evaluation for months or years while the underlying pathology worsens.
Regenerative Injections: Promising, but Not a Substitute for Structural Correction
Another rapidly expanding area is intra-articular regenerative therapy, including platelet-rich plasma (PRP), platelet-rich fibrin (PRF), sodium hyaluronate, and arthrocentesis-based protocols. Early evidence, particularly for PRP and arthrocentesis in TMJ osteoarthritis, is encouraging. These approaches can reduce inflammation, preserve cartilage in certain cases, and delay progression.
They are not, however, a cure for structural disease. A TMJ with a severely dislocated disc, a resorbing condyle, or an ankylosed joint will not be rebuilt by injections. Patients sometimes cycle through PRP, Botox, hyaluronic acid, and arthrocentesis over several years before an accurate surgical diagnosis is finally made — often by which time the surrounding jaw anatomy, airway, and bite have also deteriorated.
This is precisely the kind of pathology Dr. Wolford’s practice exists to address. When TMJ disease is advanced, the joint pathology and the jaw skeletal position are almost always intertwined — and treating one without the other leads to relapse. That’s the principle behind concomitant TMJ and orthognathic (corrective jaw) surgery: the recognition that the joint, the airway, and the jaw alignment are a single functional system.
When Advanced Surgical Evaluation Is the Right Answer
So how do patients know when they’ve crossed out of “conservative-care territory” and into the zone where a maxillofacial surgical evaluation is warranted? The following clinical patterns are red flags that an expert opinion is appropriate:
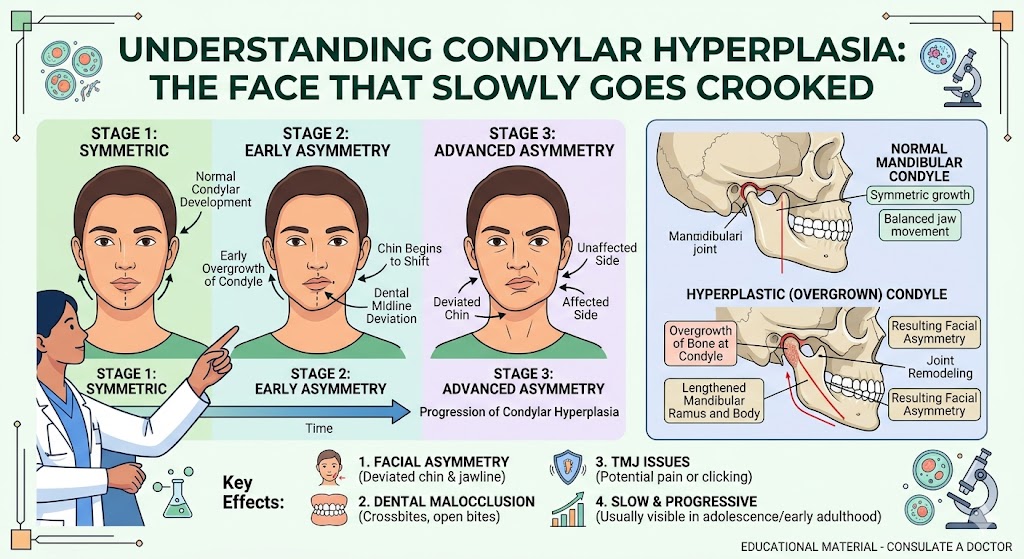
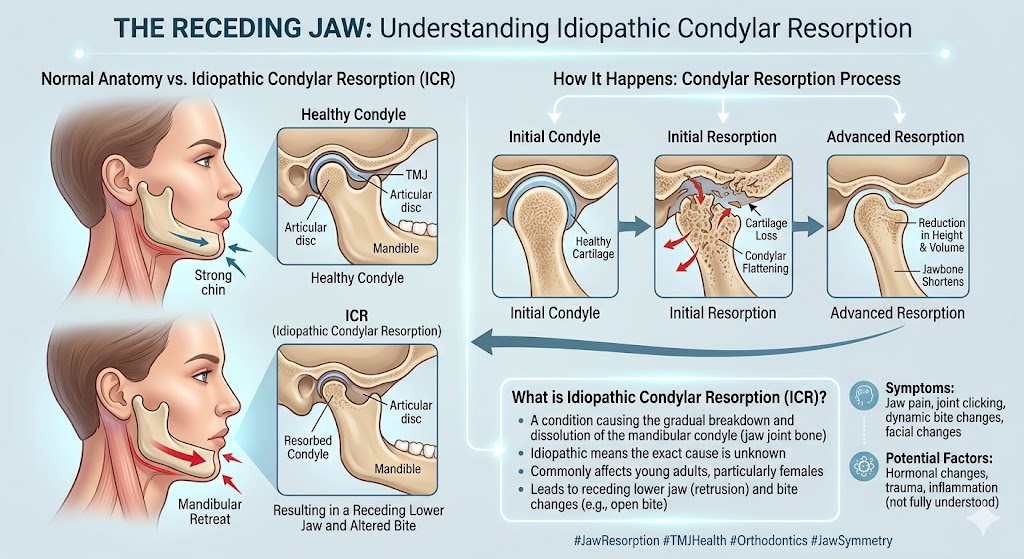
Progressive bite change over months or years. A bite that is actively shifting — especially an open bite that is opening further, or a mandible that is retruding — is often a sign of condylar resorption. This is a structural process in which the jaw joint bone is being lost, and it will not be reversed by splints. Conditions like Adolescent Internal Condylar Resorption (AICR), TMJ reactive arthritis, and connective tissue and autoimmune disease involvement of the TMJ all present this way.
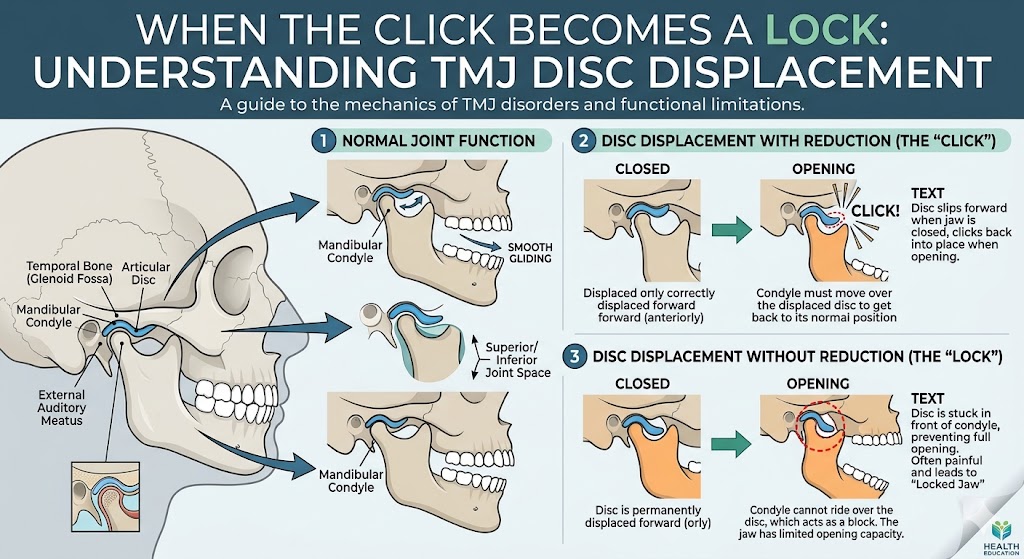
Severe limited opening or jaw locking. Chronic closed-lock, inability to open more than 25 millimeters, or a joint that has fused (ankylosis) represents end-stage internal derangement or TMJ ankylosis. These patients need imaging, an MRI evaluation, and a surgical plan — not another splint adjustment.
Failed prior jaw surgery. Patients who had orthognathic surgery years ago and have since developed pain, relapse, or worsening function often have an undiagnosed TMJ component that was missed the first time. Dr. Wolford has performed more orthognathic revision surgeries than any other maxillofacial surgeon worldwide precisely because this population is so often underserved.
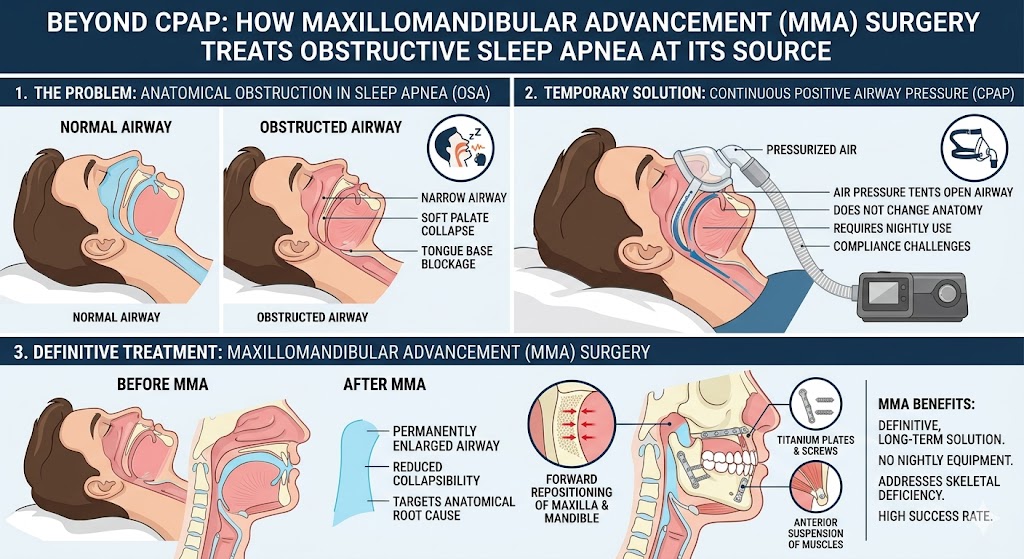
Co-existing sleep apnea and jaw deformity. If jaw pain coexists with snoring, witnessed apneas, daytime fatigue, or a diagnosis of obstructive sleep apnea, the airway and the jaw should be evaluated together. A systematic review and meta-analysis of 31 studies confirmed that maxillomandibular advancement (MMA) produces the highest success rate of any current surgical treatment for OSA, with apnea-hypopnea index reductions averaging more than 40 events per hour. For a subset of TMJ patients — particularly those with retrognathic (recessed) jaws — the same surgery that rebuilds the airway can also address the joint and bite simultaneously.
Post-traumatic joint injury. A prior facial fracture, sports injury, or whiplash event can cause long-term TMJ trauma sequelae that do not respond to conservative care and require reconstructive planning.
Systemic inflammatory or autoimmune disease. Patients with rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, lupus, scleroderma, or other connective tissue disease frequently have TMJ involvement that behaves very differently from standard TMD and often requires a total TMJ replacement when the joint has been destroyed by inflammatory disease.
Why 2026 Is Actually a Good Year to Get Evaluated
The same research wave that is producing digital therapeutics and regenerative tools is also producing dramatic progress in surgical planning and execution. Virtual surgical planning — once a novelty — is now standard in complex TMJ and orthognathic cases. Three-dimensional imaging, patient-specific implant design, and computer-guided osteotomies have made previously difficult revision cases significantly more predictable. Recent case reports even document MMA successfully performed on patients with previously reconstructed mandibles, using virtual planning as well as patient-specific osteosynthesis — a level of customization that was barely imaginable a decade ago.
Combined with patient-specific total joint prostheses and enhanced understanding of how the TMJ, airway, and facial skeleton interact, today’s outcomes for appropriately selected patients are better than at any point in the history of the specialty. For patients with advanced disease, this is genuinely a better time to be evaluated than five years ago. The tools are sharper, the diagnostics are more precise, and the planning is more individualized.
The Patient’s Task: Get the Right Diagnosis First
If there is one theme uniting every piece of 2026 TMJ research — the TMD IMPACT Initiative, the precision-medicine literature, the biomarker work, the surgical imaging advances — it is the shift toward accurate phenotyping. TMD is not a single disease. It’s a family of very different conditions with very different prognoses, and lumping them together is what has historically caused both over-treatment (surgery when splints would have sufficed) and under-treatment (years of splints for patients who needed reconstruction a long time ago).
If you have been managing TMJ symptoms for more than a year with incomplete relief, or if your symptoms are progressing, the single most valuable step you can take is getting a precise diagnosis from a surgeon whose daily practice is complex TMJ and orthognathic disease. A good starting point is a thorough TMJ and airway evaluation, including MRI imaging to assess the disc and surrounding soft tissues, and a careful review of your full history. Dr. Wolford’s office offers a free 15-minute telephone consultation at 214.828.9115 for patients who want to explore whether they satisfy the profile for specialized evaluation, and the TMJ Pain Questionnaire on the site is a useful self-assessment starting point.
The Bottom Line
The 2026 TMJ research landscape is the most promising it has ever been — and that’s true for both conservative and surgical patients. The TMD IMPACT Initiative, the flood of federal funding, the emergence of digital therapeutics, and the refinement of regenerative injections all represent real progress, especially for the large majority of TMD patients who will benefit from better-defined conservative care.
But for patients whose disease has moved past that threshold — those with progressive condylar resorption, ankylosis, end-stage arthritis, failed prior surgery, or combined airway and jaw deformity — the progress that matters most is the one happening in the operating room. More precise imaging, patient-specific implants, virtual surgical planning, and surgeons with decades of focused experience in revision and reconstructive cases have made today’s outcomes genuinely life-changing.
The worst outcome in 2026 is the same as it was in 2016: a patient with treatable structural disease spending years cycling through symptom-management tools while the underlying anatomy quietly worsens. The best outcome is the one the research itself is pointing toward — the right diagnosis, matched to the right treatment, delivered at the right time.
If you’ve been on that cycle and you’re not sure which category you fall into, getting a specialized evaluation is the single most useful thing you can do this year.
Further Reading on drlarrywolford.com