Waking up exhausted after a full night’s sleep is not just frustrating—it is a warning sign. For the nearly 30 million adults in the United States diagnosed with obstructive sleep apnea (OSA), according to the American Academy of Sleep Medicine (AASM), daily fatigue is one symptom of a far more serious condition. OSA occurs when the upper airway repeatedly collapses during sleep, cutting off oxygen to the brain and body. The consequences extend well beyond feeling tired: untreated OSA is clinically associated with hypertension, stroke, heart disease, and type 2 diabetes, as noted by the Mayo Clinic.
For many patients, the standard treatment—Continuous Positive Airway Pressure (CPAP) therapy—offers meaningful relief. But it comes with a major limitation: adherence. According to the American Association of Oral and Maxillofacial Surgeons (AAOMS), fewer than 50% of patients on CPAP are adequately treated, defined as using CPAP for 4 or more hours on 70% of nights. A machine you cannot tolerate wearing is not a solution—it is a burden.
This is precisely where maxillofacial surgery comes into play. For patients whose OSA stems from skeletal anatomy—the structure of their jaws—surgical intervention can do what no mask ever can: correct the root cause. This article examines how jaw structure contributes to obstructive sleep apnea, what surgical options exist, and why expertise matters when choosing a surgical provider.
The Anatomy of Obstruction: How Your Jaw Affects Your Airway
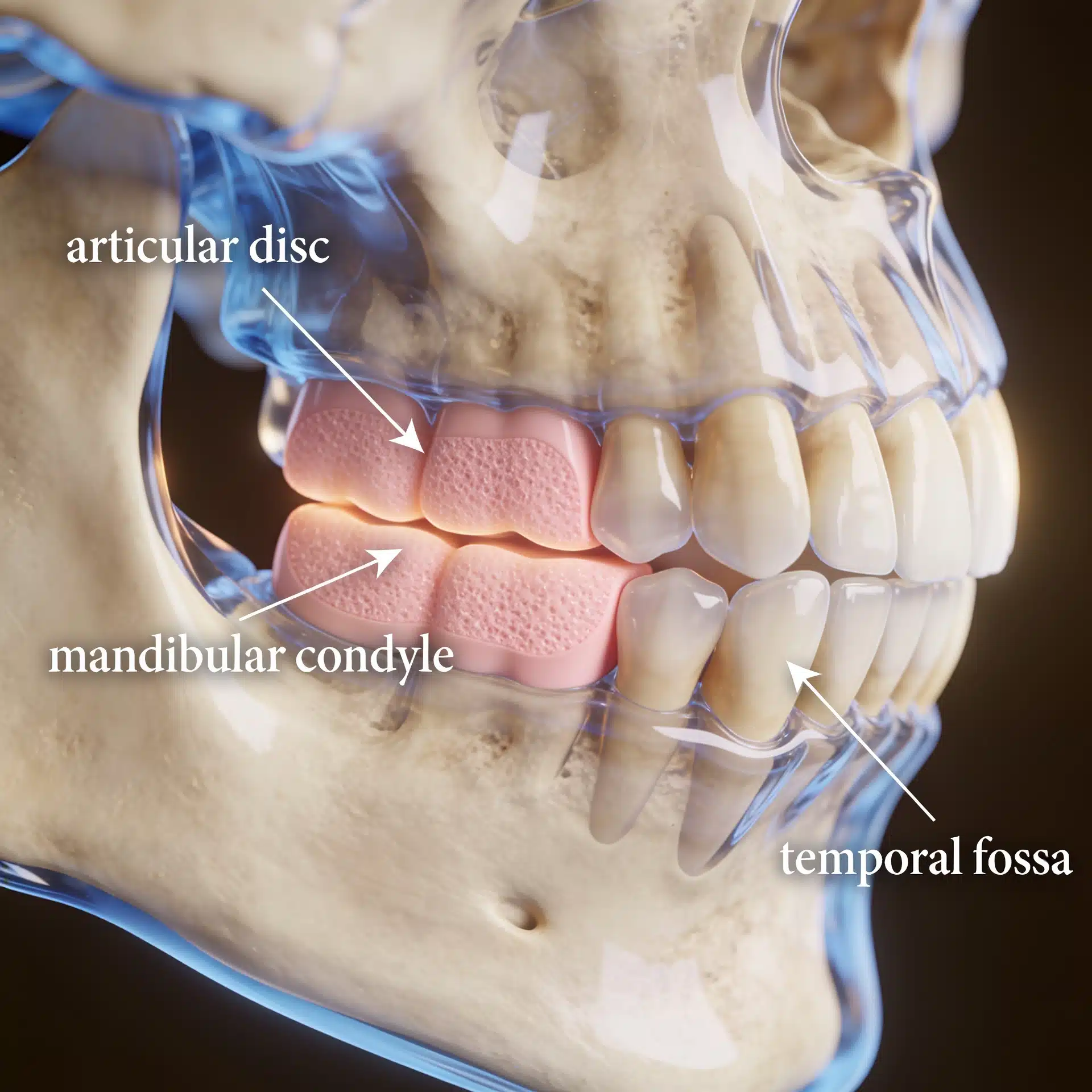
To understand how surgery can resolve sleep apnea, it helps to understand why the airway collapses in the first place.
OSA is not always a soft-tissue problem. In many patients, the skeleton is to blame. When the upper jaw (maxilla) and lower jaw (mandible) are recessed—positioned too far back—they leave little space at the back of the throat. This narrow airway means even minor changes during sleep can cause problems.
Muscles relax naturally during sleep. The tongue and soft palate lose some forward support. With a recessed jaw, there is not enough bone for these tissues to rest on. They then fall backward and can collapse against the airway wall. This results in partial or complete obstruction—an apneic event—which deprives the body of oxygen and interrupts sleep. The brain senses the oxygen drop and causes brief arousals to restore breathing. This cycle can repeat hundreds of times per night.
This skeletal pattern is often paired with other visible characteristics, such as a receding chin, a “weak” jawline, or an overbite. These facial features are not simply aesthetic concerns; they are outward indicators of an airway that may be structurally compromised from the outset.
No amount of air from a CPAP machine changes your bones. It can keep the airway open for a while, but once you remove the mask, the problem persists. For people whose OSA is clearly caused by their bones, fixing the bones is a very different—and possibly better—way to treat sleep apnea.
Surgical Solutions: Maxillomandibular Advancement and Beyond
The gold standard surgical treatment for skeletal obstructive sleep apnea is Maxillomandibular Advancement (MMA). Outside of tracheostomy, the AAOMS considers MMA to be the most effective therapy for severe OSA—a designation it has earned through a strong body of clinical evidence.
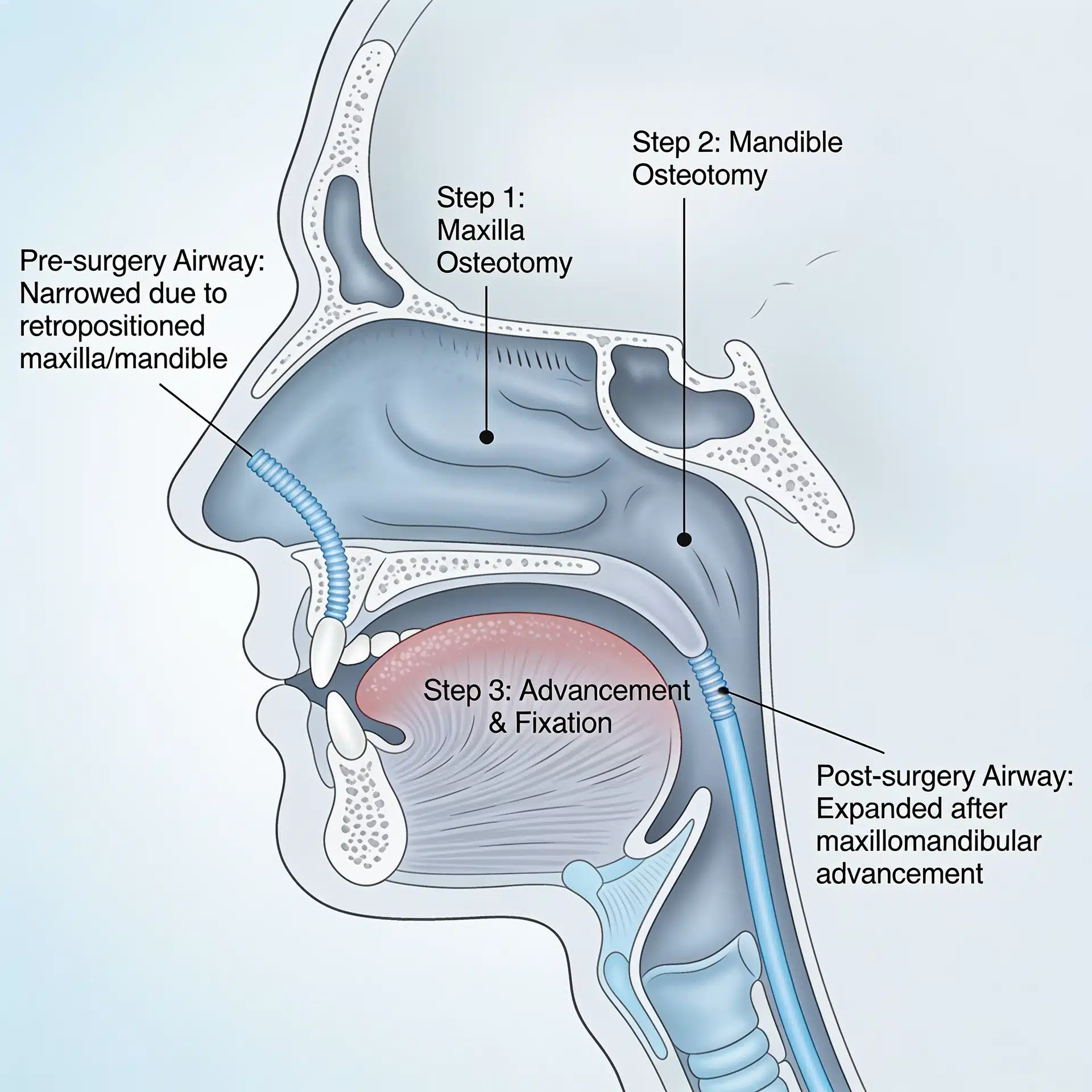
How MMA Works
During MMA surgery, the oral and maxillofacial surgeon makes precise osteotomy cuts in both the maxilla and mandible. Both jaws are then physically moved forward and secured in their new positions with surgical hardware. Because the tongue and soft palate are structurally attached to the jawbones, advancing the jaws pulls these soft tissues forward, dramatically enlarging the posterior airway space. The result is a permanent, non-device-dependent structural expansion of the airway.
The clinical evidence supporting MMA is substantial. A 2021 systematic review and meta-analysis published in PubMed analyzed outcomes across 20 MMA studies and found that patients experienced a significant reduction in the Apnea-Hypopnea Index (AHI)—the primary clinical measure of OSA severity—of 46.2 events per hour on average. The pooled surgical success rate was 85.0%, and the surgical cure rate was 46.3%. A separate meta-analysis confirmed that success rates for MMA remain above 80% even in patients with obesity. The AAOMS further notes that MMA has a high success rate, often eliminating the need for a CPAP machine entirely.
The 2021 AASM clinical practice guideline on surgical referral for adults with OSA provides strong recommendations for discussing surgical referral with patients who are intolerant of or unaccepting of PAP therapy, and conditional recommendations for those with persistent, inadequate adherence due to pressure-related side effects. The guideline designates oral and maxillofacial surgeons, alongside otolaryngologists, as qualified sleep surgeons for this patient population.
Additional Surgical Considerations
MMA is often the main and most helpful surgery, but your surgeon may look for other reasons why your airway is blocked. These can include:
- Nasal turbinate reduction to address nasal obstruction that increases airway resistance
- Genioplasty (chin advancement) to help support the airway and improve how the face looks
- Checking and treating the jaw joint to make sure it can handle the jaw movement without causing problems
Each additional procedure is chosen for the individual patient. Decisions are based on anatomy, imaging, and clinical findings. The AASM guideline notes that choosing surgery “is a complex decision requiring an informed discussion of risks and benefits.” Decisions must incorporate the patient’s anatomy and personal values.
Comprehending the Risks
MMA is a major surgical procedure and has a higher complication profile than soft-tissue surgeries. The same 2021 meta-analysis reported a major complication rate of 3.2% for MMA. Possible long-term side effects—reported at low incidence—include mandibular paresthesia (temporary or permanent numbness along the jaw), minor alterations in facial appearance, and changes in dental occlusion. These risks underscore why surgical expertise and preoperative planning are not optional—they are foundational to a safe and successful outcome.
Dr. Larry Wolford: Precision, Experience, and Innovation in Airway Surgery
Performing MMA well takes more than technical skill. The surgeon must expand the airway, protect facial structures, maintain a good bite, and keep the jaw joints healthy. Balancing these demands requires knowledge and experience that few surgeons possess.
Dr. Larry M. Wolford, DMD, is a Clinical Professor of Oral and Maxillofacial Surgery and Orthodontics at Texas A&M University Health Science Center, Baylor College of Dentistry, and practices at Baylor University Medical Center in Dallas, Texas. He is a Diplomat of the American Board of Oral and Maxillofacial Surgery with over 40 years of experience in complex surgery and more than 185 published scientific papers. Sixty-five percent of his practice consists of patients referred from across the United States and internationally—a reflection of the confidence other clinicians place in his abilities.
Dr. Wolford is recognized internationally as a leading innovator in orthognathic surgery, TMJ reconstruction, and maxillofacial revision surgery. He is especially known for his refinement of the counter-clockwise rotation technique, an advanced MMA approach in which the occlusal plane—the angle of the bite—is rotated rather than simply translated forward. This rotation achieves greater posterior airway expansion than standard advancement alone, while simultaneously producing a more aesthetically balanced facial profile. The technique is considered a hallmark of advanced-level OSA surgery.
His pre-surgical protocol uses 3D virtual planning to simulate airway results before surgery. TMJ stability is checked before proceeding. Nasal procedures are combined if needed. This approach aims to treat the entire patient, not just a single measurement. Wolford has trained hundreds of surgeons through fellowships at Baylor University and Texas A&M. Oral and maxillofacial specialists often refer their toughest cases to him. Many of these patients have already had unsuccessful surgeries elsewhere.
With a clear picture of what jaw surgery involves and who performs it, we next examine: Who is a candidate for jaw surgery for sleep apnea?
Not every patient with OSA requires or is suitable for surgical intervention. The most appropriate candidates usually meet one or more of the following criteria:
- CPAP intolerance or non-acceptance: Patients who cannot tolerate or consistently use PAP therapy despite appropriate trials and interventions
- Skeletal jaw abnormalities: Patients whose imaging and clinical evaluation reveal mandibular and/or maxillary retrusion, causing airway narrowing
- Moderate-to-severe OSA: Patients with AHI values that reflect significant disease burden and elevated cardiovascular risk
- Failed soft tissue surgery: Patients who have undergone previous upper airway soft tissue procedures without achieving adequate relief
- Malocclusion or bite dysfunction: Patients whose jaw misalignment creates both operative and airway-related consequences
A detailed clinical evaluation—including physical examination, sleep study results, and imaging such as cone beam CT or lateral cephalometric radiographs—is required to determine candidacy. The AASM guideline emphasizes that “a standard surgical consultation includes a detailed anatomic assessment for surgical treatment, occasionally using tools unavailable to the average health care provider.” This evaluation serves as the basis for individualized surgical planning and informed consent.
Frequently Asked Questions
Is jaw surgery a permanent cure for sleep apnea?
For many patients, MMA produces a durable, long-term resolution of OSA by permanently expanding the skeletal airway. Clinical data show surgical cure rates approaching 46% and success rates exceeding 85%. Individual outcomes depend on the severity of OSA, the degree of advancement achieved, and patient anatomy. A thorough pre-operative evaluation helps establish realistic expectations.
How long is the recovery after MMA surgery?
Recovery usually involves a period of dietary restriction (soft foods initially) and follow-up visits to monitor healing and occlusal stability. Swelling and temporary numbness along the jaw are common in the early weeks. Most patients return to normal daily activities within several weeks, though full bony healing takes several months.
Will jaw surgery affect my appearance?
In many patients with skeletal retrusion, advancing the jaws actually improves the facial profile, producing a better-balanced, more defined jawline and chin. Dr. Wolford’s use of counter-clockwise rotation is specifically created to optimize both airway and cosmetic outcomes simultaneously.
What if I have both sleep apnea and TMJ problems?
Dr. Wolford is uniquely qualified to address concomitant TMJ pathology and OSA in the same surgical setting. His protocols include pre-operative TMJ assessment, and his practice specializes in complex cases involving both jaw joint dysfunction and airway compromise.
Can I still try CPAP after surgery if needed?
Yes. MMA surgery that markedly reduces OSA severity often lowers CPAP pressure requirements, even when complete resolution is not achieved—boosting patient tolerance and adherence to therapy. This is recognized in the AASM guideline as a clinically significant secondary benefit of upper airway surgery.
Make the First Step Toward Lasting Relief
Obstructive sleep apnea is a progressive condition. Left untreated—or inadequately managed—it compounds cardiovascular risk, damages cognitive function, and systematically undermines quality of life. A CPAP machine that sits unused on a nightstand offers no protection.
For patients with skeletal anatomy underlying their OSA, maxillomandibular advancement surgery offers a treatment approach that addresses the underlying cause. The evidence supporting MMA’s efficacy is well-established. The clinical guidelines support surgical referral. What remains is identifying the right surgeon.
Dr. Larry Wolford’s practice at Baylor University Medical Center in Dallas, Texas, offers a free initial telephone consultation for prospective patients. Contact Dr. Wolford’s office at 214.828.9115 or schedule an appointment online to discuss your airway anatomy and explore whether surgical treatment is the right option for you.