A few decades ago, if you needed complex jaw or facial surgery, your surgeon worked from two-dimensional X-rays, plaster models of your teeth, and a lot of hard-won experience bent over a light box. The plan lived partly on paper, partly in the surgeon’s head, and the final adjustments happened in the operating room while you were asleep — titanium plates bent by hand to fit the bone in front of them, best judgment made in real time.
That world is disappearing. And for patients who need serious jaw surgery, that’s genuinely good news.
In 2026, the tools have caught up with the ambition. 3D printing, virtual surgical planning, and patient-specific implants have moved from “interesting research curiosity” to routine — and they’re quietly rewriting what’s possible in maxillofacial surgery. If you’re facing a jaw procedure, a TMJ replacement, or a complex revision, there are things happening now that weren’t happening five years ago. It’s worth understanding what they are and why they matter.
The Short Version
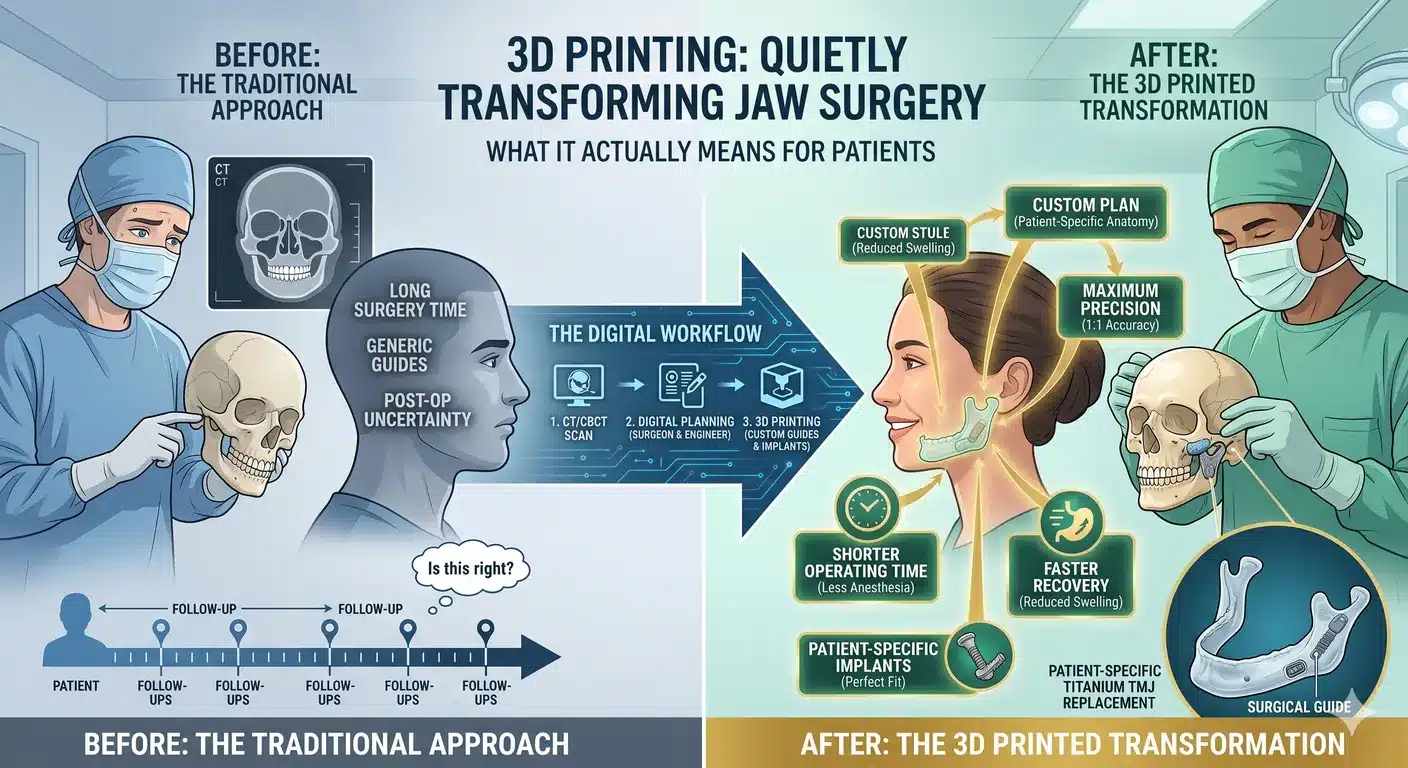
Instead of a surgeon guessing, bending, and adjusting during surgery, a 3D-printed, patient-specific approach lets the entire operation be planned on a computer model of your exact anatomy — weeks before you ever walk into the OR. Cutting guides get printed to match your bone. Plates and implants are custom-made to fit you and only you. The surgery itself becomes more of an execution of a precise plan than a set of in-the-moment decisions.
The results, according to a 2025 meta-analysis of clinical outcomes with 3D-printed patient-specific implants, are shorter operating times, better anatomical fit, fewer complications, and higher implant survival. A separate scoping review covering studies from 2015 through early 2025 found the same pattern — reduced surgical time, high implant survival, and better functional outcomes for speech and chewing, with complication rates staying low.
That’s a real shift. Let’s break down what’s actually happening and what it means if you’re the patient on the table.
How a Jaw Surgery Used to Get Planned
Traditional maxillofacial surgery relied on a stack of tools that, looking back, feel almost quaint. You’d get a panoramic X-ray and a cephalometric X-ray — two flat 2D images of a deeply 3D problem. Your dentist or orthodontist would take impressions of your teeth to make plaster models. The surgeon would hand-articulate those models, saw them apart, reposition the fake jaws where they should go, and glue them back together with wax.
That wax model became the surgical plan. During the operation, the surgeon would reference it, cut the real bones along similar lines, and reposition them into an acrylic splint that had been made to match the wax model’s new bite.
It worked. Millions of successful jaw surgeries were done this way, and experienced surgeons got extraordinary results with it. But the system had real limits. You couldn’t truly see the airway. You couldn’t predict the soft tissue change. Complex asymmetries got flattened into approximations. And every hardware piece — every plate, every screw, every reconstruction device — came in standard shapes that had to be bent, trimmed, and wrestled into fit during the surgery itself.
As the clinical literature has pointed out, that repeated bending introduces internal stress into titanium plates, which can contribute to implant fatigue, screw loosening, and — in some cases — later failure. It was a solvable problem, but you had to solve it at every surgery.
What’s Different Now
The modern workflow starts the same way every major maxillofacial case now starts: a thin-slice CT scan and intraoral scanning of your teeth. That data gets imported into CAD software — the same class of software used in aerospace and industrial design, adapted for medicine. From there, everything changes.
You get a digital twin. Your surgeon is now looking at a 3D reconstruction of your actual skull, jaws, teeth, airway, and TMJs on a screen. They can rotate it, cut through it, take measurements that are impossible on physical models, and visualize problems that were previously hidden.
The surgery gets rehearsed before it happens. Virtual surgical planning (VSP) lets the surgeon perform the entire procedure in the computer first — making the cuts, moving the bone segments, placing them in the ideal new position, checking how the bite fits, looking at how the airway changes, verifying the symmetry. Problems get solved at the computer instead of in the operating room. Surgeons and engineering teams work through the plan together, iterating until it’s right.
Cutting guides are 3D-printed to match your bone. Once the plan is finalized, the lab prints sterile, patient-specific cutting guides that fit onto your jaw in exactly one way — the correct way. These guides tell the surgeon where every cut goes, at what angle, and how deep. It removes one of the biggest sources of variability in jaw surgery: freehand osteotomies.
Plates and implants are custom-manufactured for you. Instead of bending a generic plate during surgery, the hardware is designed in the virtual plan and then 3D-printed or milled from medical-grade titanium (or, in some cases, PEEK polymer or bioresorbable material) to match the exact contours of your new anatomy. Titanium is typically preferred for load-bearing reconstructions of the mandible and orbit, while PEEK is often chosen for aesthetic or revision cases where its flexibility and radiolucency matter. Bioresorbable materials are increasingly used in pediatric cases to avoid the need for later revision.
The surgery itself becomes faster and more precise. Because the planning has already happened, the surgical team spends less time deciding and more time executing. The evidence backs this up: the 2025 meta-analysis found consistent reductions in operative time alongside improved implant integration and outcomes.
Why This Matters More in Complex Cases
For straightforward jaw surgery — a single-jaw advancement in a cooperative, healthy patient with clean anatomy — a great surgeon can get excellent results with or without elaborate 3D planning. The real transformation is in the cases where the old tools were always struggling.
Revision surgery. Patients who’ve had prior jaw surgery with incomplete or failed results are one of the hardest groups in all of maxillofacial medicine. The anatomy is already altered. Scar tissue makes everything harder to read. The usual landmarks are distorted. Dr. Wolford’s practice has long been recognized globally for complex orthognathic revision surgery, precisely because these are the cases that demand the most from both the surgeon and the planning technology.
3D planning has changed the revision game. Old hardware can be visualized, worked around, or replaced. The actual outcome of the original surgery can be compared to what was intended, and a corrective plan can be built that respects what’s already there. Patient-specific hardware means the new plates don’t have to be wrestled around existing implants or bent to fit altered bone.
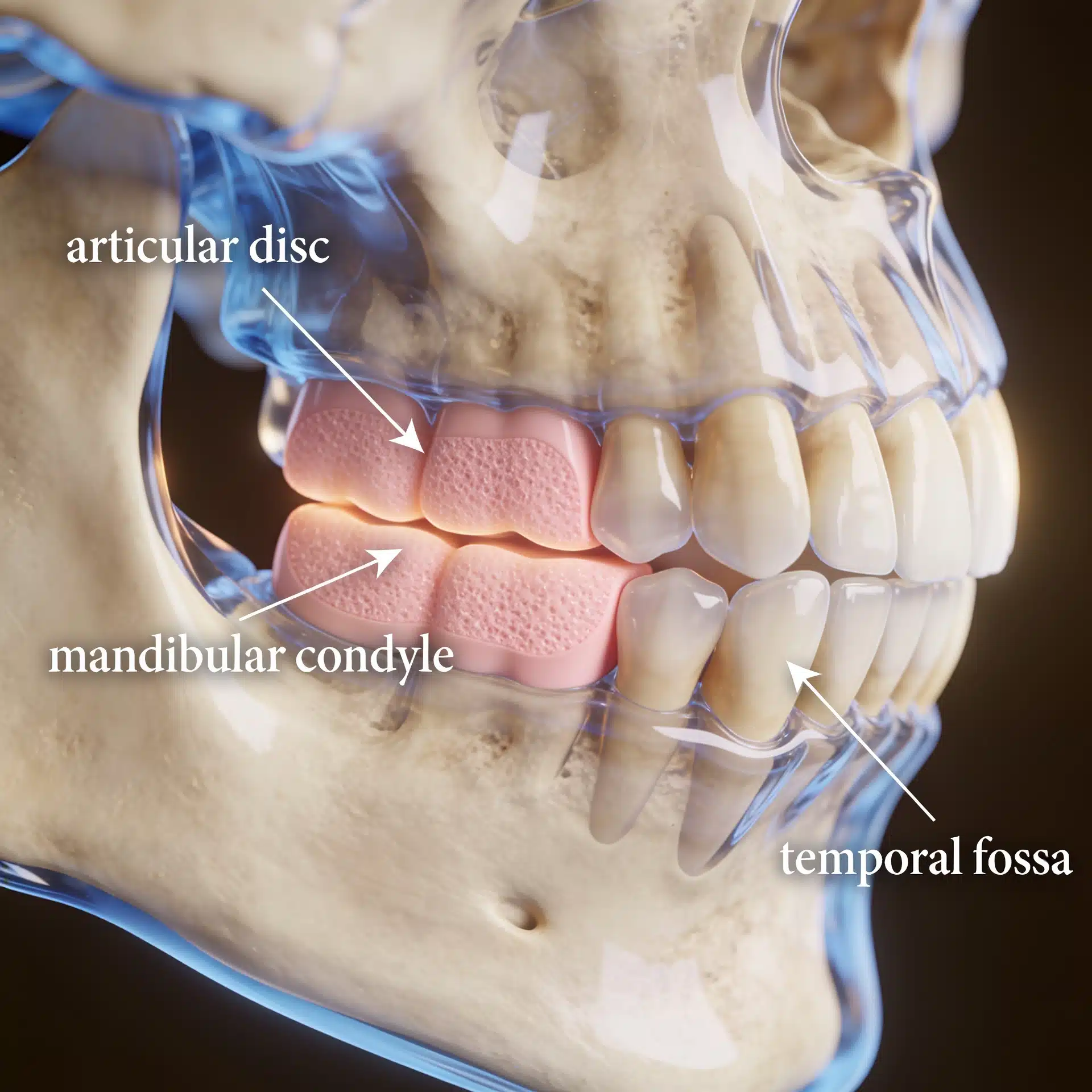
TMJ replacement. Total TMJ replacement is arguably the case where custom hardware matters most. The temporomandibular joint is small, complex, and highly individual. A stock prosthesis has to be approximated to the patient’s anatomy; a patient-specific prosthesis is designed to match it. For patients with end-stage TMJ disease — severe arthritis, ankylosis, condylar resorption, or the destructive joint damage that can accompany connective tissue and autoimmune disease — custom prostheses make an enormous difference in fit, function, and longevity.
Jaw asymmetry. Mandibular condylar hyperplasia and other asymmetric growth disorders produce jaws that aren’t mirror images of themselves. Planning that kind of correction on flat X-rays is limiting. Planning it in 3D, with virtual movements that can be measured to the millimeter, changes how predictable the result is.
Combined TMJ and orthognathic cases. When a patient has both jaw deformity and TMJ pathology — which is more common than most people realize — concomitant TMJ and orthognathic surgery is the right answer. These cases benefit hugely from integrated virtual planning, because the joint reconstruction and the jaw repositioning have to be solved as one problem, not two.
Craniofacial reconstruction. For patients with craniofacial deformities, post-traumatic reconstruction, or congenital syndromes, 3D-printed patient-specific implants have been genuinely transformative. Mirror-image designs can be used to reconstruct one side of the face based on the other. Complex defects can be filled with hardware that looks, in the CT scan, like it grew there.
What the Research Is Showing in 2026
The evidence base has matured fast. A few findings worth knowing about:
The 2025 systematic review and meta-analysis of 183 patients across eight studies found that 3D-printed patient-specific implants delivered better anatomical fit and higher surgical efficiency than traditional approaches in maxillofacial reconstruction, with a favorable safety profile.
A January 2026 paper on 3D-printed patient-specific surgical instruments and implants described craniomaxillofacial titanium plates and implants as already “routine” — a word that matters, because it signals that the technology has crossed from experimental to standard of care in sophisticated centers.
The scoping review covering ten years of literature on patient-specific implants for intraoral and maxillofacial reconstruction concluded that there’s no major difference in fit or longevity between milled and printed implants — both work, both last, both deliver. It also highlighted where the field is going next: bioprinting and tissue engineering approaches that could eventually produce biologically integrated reconstructions rather than purely mechanical ones.
What remains genuinely hard, the literature agrees, is cost, regulatory approval timelines, and long-term validation. Patient-specific implants still take longer to produce than pulling a stock plate off a shelf. They still need to be cleared through proper regulatory channels. And the really exciting frontiers — 3D-printed living tissue, bioactive scaffolds — are still mostly in research.
But for the tools that exist right now? They work, and they’re changing outcomes.
What Patients Should Understand
If you’re heading toward maxillofacial surgery in the current era, a few things are worth knowing about how the technology affects your care.
Good planning takes time — and that’s a feature, not a bug. A properly planned jaw surgery with patient-specific hardware typically requires several weeks between the decision to operate and the actual surgery date. CT scans have to be done. Models have to be built. The plan has to be developed, reviewed, refined, and finalized. Hardware has to be manufactured and sterilized. If a practice is rushing that process, it’s not a good sign. If they’re taking time to do it properly, it’s a sign they’re doing it right.
You should ask to see your plan. One of the best uses of virtual surgical planning isn’t surgical — it’s communicative. The 3D model lets your surgeon walk you through exactly what’s going to happen, why, and what it should look like afterward. You can see the before and the predicted after. You can ask questions about things you couldn’t have asked about ten years ago. That’s your plan. See it.
Not every case needs the full technology suite. A simple third molar removal doesn’t need patient-specific implants. A routine sleep apnea evaluation doesn’t need a full virtual surgical workup. The question is whether your specific case is complex enough to benefit — and if it is, whether your surgeon has the infrastructure and experience to use the tools well.
The surgeon still matters more than the technology. This is the most important point. 3D printing, VSP, and patient-specific implants are powerful tools, but they’re tools. A well-planned operation performed by an inexperienced surgeon will still produce worse results than a carefully thought-through operation performed by an expert surgeon. The technology amplifies what the surgeon brings to the table — it doesn’t replace it. When you’re evaluating where to have complex jaw surgery, you’re still evaluating the surgeon first, and the technology second.
The learning curve is real. Using these tools well requires training, repetition, and genuine expertise in the underlying surgery. Centers that have been doing high-volume complex jaw and TMJ work for years — and have been building their digital workflows over that same time — are in a different place than practices that are just starting to adopt the technology. That experience shows up in the planning choices, the execution, and the outcomes.
Where Dr. Wolford’s Practice Fits In
Dr. Wolford has been at the center of advanced maxillofacial surgery for decades, with a body of published research covering everything from airway space changes after orthognathic surgery to the long-term effects of double-jaw surgery on obstructive sleep apnea. His Virtual Surgical Treatment Planning workflow is a core part of how complex cases get mapped out before surgery.
The practice sees a high volume of the cases that benefit most from this kind of planning — revision jaw surgery, complex TMJ reconstruction, total TMJ replacement, and combined TMJ-orthognathic work for patients who’ve been told elsewhere that their problems were too complicated to fix. In those situations, the combination of decades of surgical experience and modern virtual planning is where the real value shows up.
Patients considering evaluation for complex jaw or TMJ surgery can reach the Dallas office for a free 15-minute telephone consultation at 214.828.9115. Self-assessment resources on the site — the TMJ Pain Questionnaire and the Airway Questionnaire for Sleep Apnea — are useful starting points before a formal consultation.
The Bottom Line
3D printing, virtual surgical planning, and patient-specific implants haven’t made maxillofacial surgery easier in the sense of “anyone can do it now.” They’ve made it more precise. Operations that used to depend on intraoperative judgment now depend on careful, collaborative planning that happens long before the first incision. Hardware that used to be bent by hand now arrives perfectly shaped for the patient it’s going into. Complex asymmetries, revisions, and reconstructions that once pushed the limits of what was possible are now routinely handled.
That’s a real change. For patients with straightforward cases, it means shorter, more predictable procedures. For patients with complex cases — the revisions, the end-stage joints, the failed prior surgeries, the asymmetric jaws, the combined pathology — it means outcomes that genuinely weren’t achievable a generation ago.
The technology isn’t the reason good outcomes happen. Good surgeons are. But the tools are now good enough that the ceiling on what’s possible has moved up substantially. For anyone facing serious jaw surgery in 2026, that’s a shift worth understanding — and worth asking about when you’re deciding where to have your care done.
Related Reading on drlarrywolford.com
- Meet Dr. Larry M. Wolford
- Virtual Surgical Treatment Planning
- Orthognathic (Corrective Jaw) Surgery
- Complex Orthognathic Revision Surgery
- Total TMJ Replacement
- TMJ Dysfunction Overview
- Mandibular Condylar Hyperplasia
- Craniofacial Deformities
- Research Publications
- Before & After Surgery Results
- Contact the Office