Medically reviewed and authored by Larry M. Wolford, DMD — Board-Certified Oral & Maxillofacial Surgeon, Dallas, TX. Last reviewed: May 2026.
Educational disclaimer: This article is for general educational purposes and is not a substitute for an individualized medical evaluation. Candidacy for any surgical procedure can only be determined through in-person examination and imaging. No outcome is guaranteed; results vary by patient.
It rarely starts dramatically. It starts with a click. Then mornings when the jaw won’t open past two fingers. Then a diet quietly narrowing to soft foods because chewing has become a negotiation with pain. Many patients spend years cycling through night guards, physical therapy, anti-inflammatories, and reassurance that “it’s just stress” — while the joint itself keeps changing. By the time some patients reach a surgeon who focuses on the temporomandibular joint, they’ve stopped expecting anyone to take the problem seriously.
That experience is common, and it is not imagined. For a specific subset of patients, the jaw joint has reached a point where conservative care can no longer restore it — and understanding why is the first step toward a real plan.
The Real Problem: End-Stage Joint Degeneration
The opponent here is not a person, a prior dentist, or “stress.” It is a disease process — and naming it precisely matters because it dictates treatment.
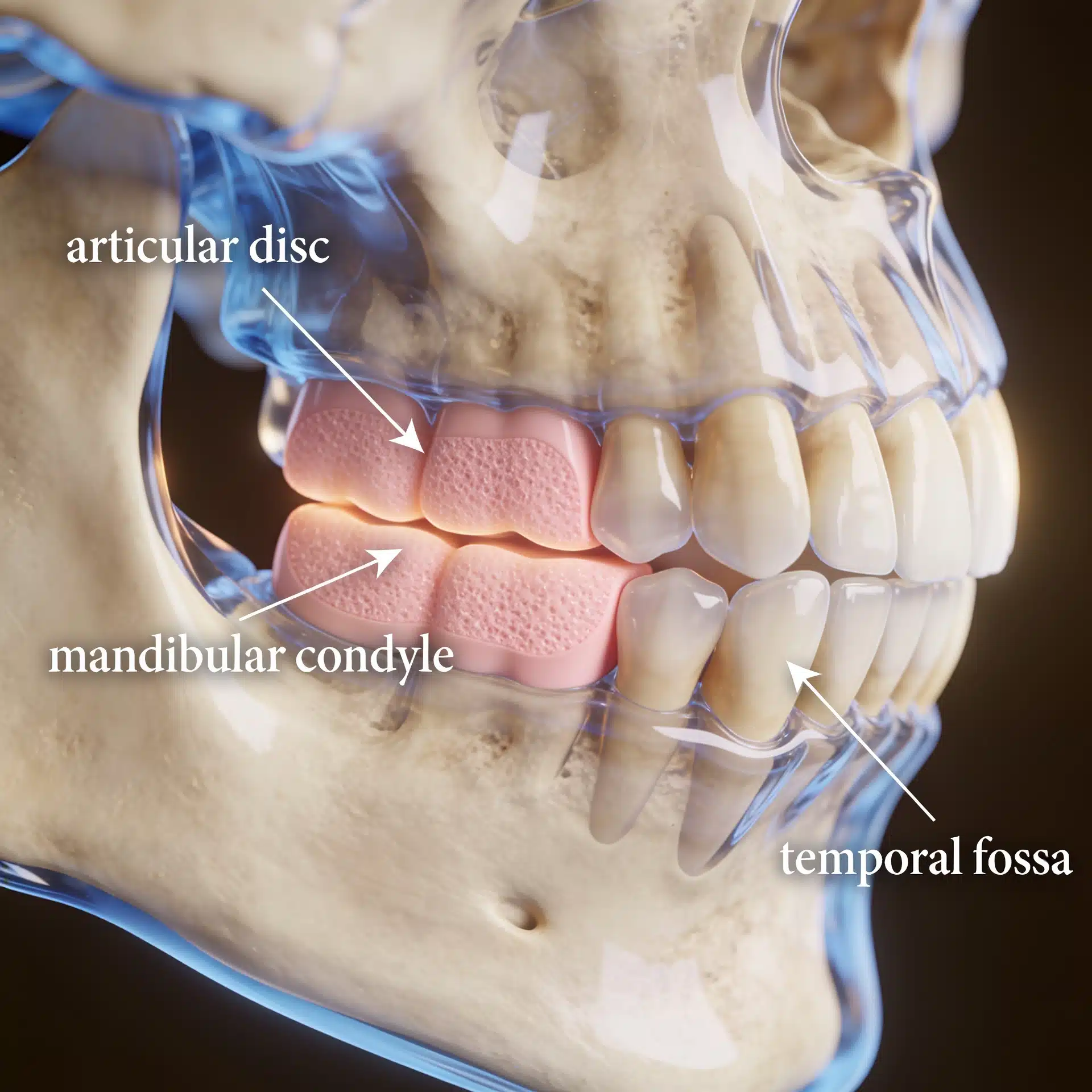
In a healthy temporomandibular joint (TMJ), a small fibrocartilage disc cushions the jaw condyle against the skull base. When that disc displaces and stays displaced, the bone surfaces it was protecting begin to bear load they were never meant to bear. (For a plain-language overview of how these joints work and the conditions that affect them, see Dr. Wolford’s TMJ dysfunction overview, and the National Institute of Dental and Craniofacial Research’s patient guide to temporomandibular disorders.) Over time this can progress to end-stage TMJ disease: degenerative joint disease (osteoarthritis), idiopathic condylar resorption, reactive or rheumatoid arthritis, ankylosis (the joint fusing with scar or bone), tumors, or a joint already damaged by prior failed surgery.
The defining feature of end-stage disease is that the joint’s own anatomy is gone or destroyed. Splints, injections, and physical therapy manage symptoms — they cannot regrow a resorbed condyle or free an ankylosed joint. That is the threshold where reconstruction enters the conversation.

What an Experienced TMJ Surgeon Brings to the Decision
The goal of a focused TMJ practice is not a guaranteed cure — no ethical surgeon can promise that. The value is diagnostic precision and surgical experience applied to a problem that is frequently misdiagnosed. TMJ pathology and jaw deformity often coexist, and treating one while ignoring the other is a common reason surgeries fail.
Dr. Wolford has spent more than 40 years concentrating on the TMJ and the jaws, has authored over 185 peer-reviewed scientific publications, helped develop techniques now used internationally (including the Mitek Anchor approach for articular disc repositioning), and has performed more patient-fitted total TMJ joint prostheses than any other surgeon in the country. That depth doesn’t change your anatomy — but it changes the quality of the diagnosis and the plan built around it. (Dr. Wolford’s comprehensive clinical article on total TMJ replacement covers the diagnostic and treatment-planning detail in depth.)
Key Takeaways
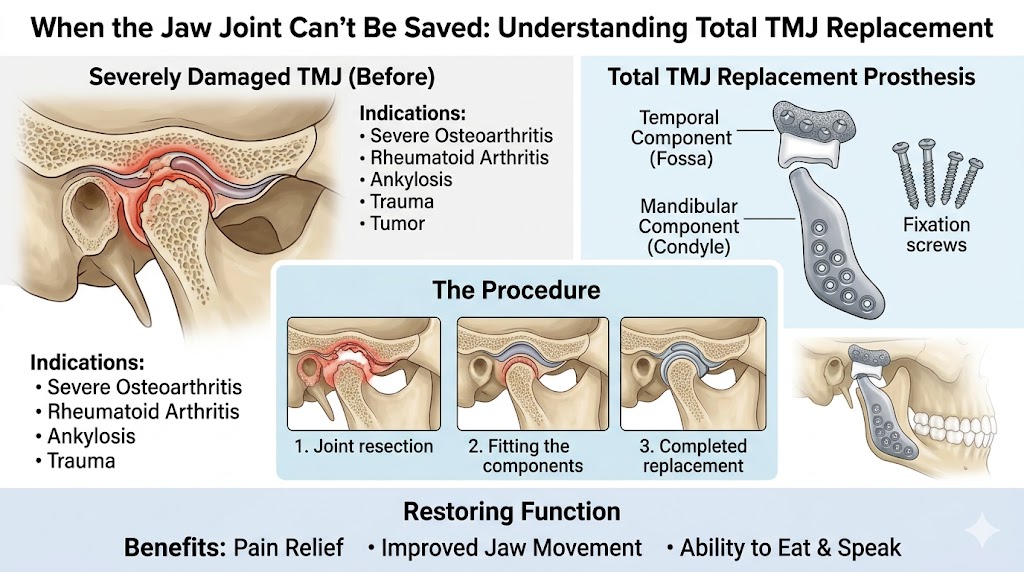
- Total TMJ replacement is for end-stage disease only — when the joint’s bone and disc are destroyed and cannot be repaired or will not respond to conservative care.
- Common indications include ankylosis, idiopathic condylar resorption, severe degenerative or inflammatory arthritis, tumors, and failed prior joint surgery.
- The modern standard is a custom, patient-fitted total joint prosthesis, manufactured from a CT scan of your specific anatomy.
- TMJ and jaw position are treated together. Reconstructing the joint without correcting jaw position is a frequent cause of poor results.
- Candidacy is individual. It requires clinical exam, cone-beam CT, and usually an MRI — not a generic recommendation.
- Goals are realistic: reduce pain, restore function and stability, and stop disease progression. Outcomes vary and are never guaranteed.
How the Decision Is Actually Made
Short answer: Total TMJ joint replacement is recommended when the joint is anatomically destroyed and lower-risk options can no longer restore function — and it is best done by reconstructing the joint and correcting jaw position in the same operation when both problems are present.
Here is the reasoning behind that answer.
The diagnosis is built on imaging, not symptoms alone. Pain is a poor map of joint damage. A thorough workup uses cone-beam CT to assess bone, and MRI to assess the disc and soft tissue. This is what distinguishes a reducible early problem from end-stage destruction. At an initial surgical evaluation — which typically lasts about two hours — the goal is a detailed written diagnosis and treatment plan, including alternatives, risks, and complications, sent to both the patient and the referring doctor.
Conservative and joint-sparing options come first when they’re viable. For earlier disease, disc repositioning (such as the Mitek Anchor technique) or other joint-preserving surgery may be appropriate. Replacement is reserved for joints that can no longer be saved.
The prosthesis is custom-made. Contemporary total TMJ reconstruction commonly uses a patient-fitted device manufactured from the patient’s own CT data, so the prosthesis matches individual anatomy rather than forcing the anatomy to fit an off-the-shelf part. Long-term published literature on patient-fitted total joint prostheses supports their use for durable function and pain reduction in appropriately selected patients. These devices are regulated as medical devices and reviewed before they reach the market; the U.S. Food and Drug Administration maintains background on TMJ implants and their oversight. For a patient-focused walk-through of the device itself, recovery, and what to expect, see Dr. Wolford’s guide to custom joint prosthetics and outcomes.
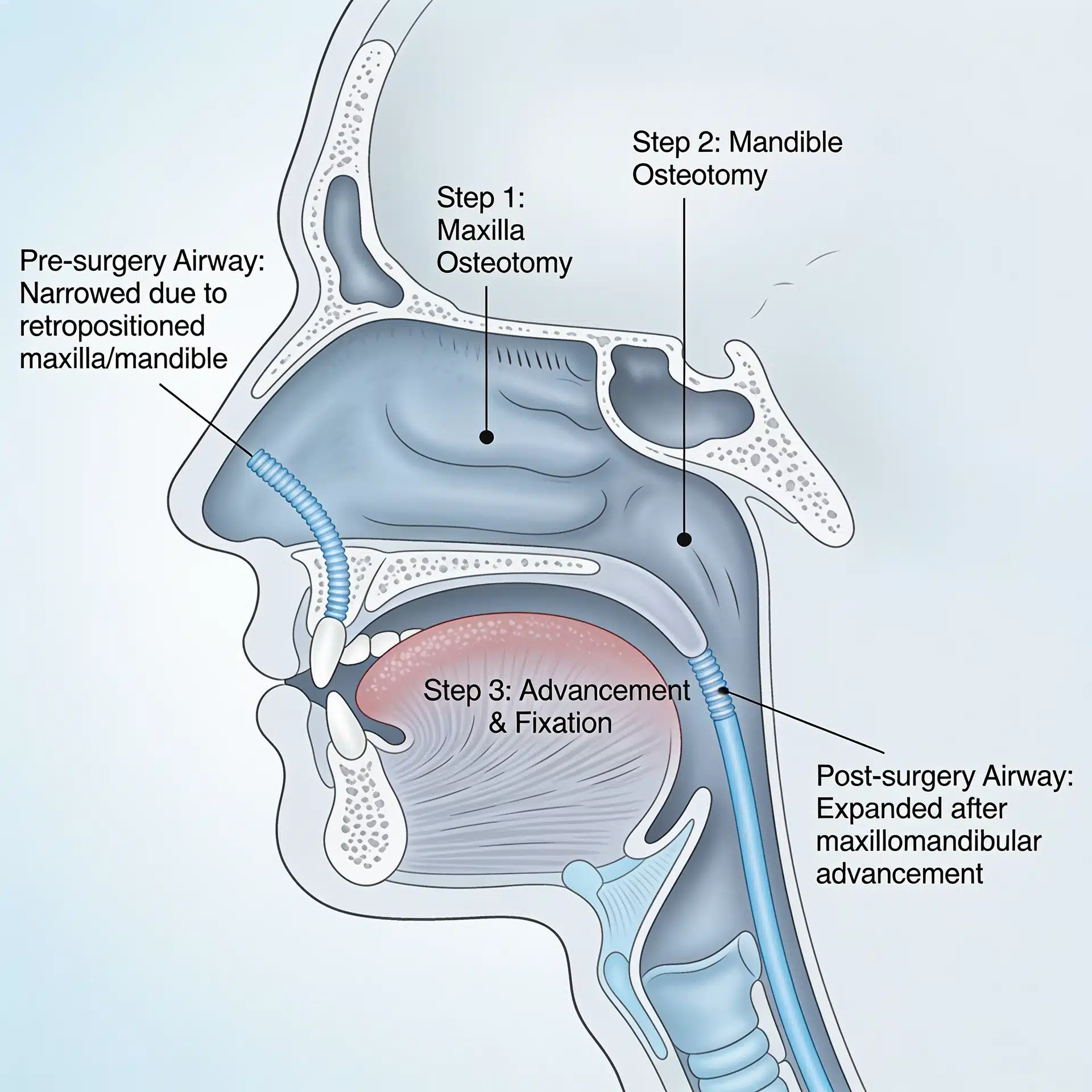
The jaw is often moved at the same time. Because TMJ pathology and jaw deformity frequently coexist, performing concomitant TMJ replacement and orthognathic (corrective jaw) surgery in a single, well-planned operation can reduce total treatment time, limit the number of hospitalizations, and produce a more stable result than staging them separately or ignoring the deformity. (Learn more about the broader scope of oral and maxillofacial surgery Dr. Wolford performs.)
Success is defined honestly. Realistic objectives are pain reduction, improved and stable jaw function, and halting disease progression — not a perfect return to a pre-disease state. Every surgery carries risk, and a candid discussion of those risks is part of informed consent.
Where This Care Happens

Dr. Wolford’s practice is located on the campus of Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 — minutes from downtown Dallas and accessible from across the Dallas–Fort Worth metroplex. Valet parking is available, with self-parking in the adjacent building.
Because this is a highly subspecialized practice, patients travel to Dallas from across the country and internationally, often flying into DFW or Dallas Love Field. Please note that all procedures for both current and new patients are performed exclusively at the Dallas office — a long-standing practice that supports consistency of care. Out-of-town patients can review what to bring and how to prepare on the patient information page. A free initial telephone consultation is available at 214-828-9115, or you can contact the office online.
Frequently Asked Questions
Am I a candidate for total TMJ replacement? Only an in-person evaluation with appropriate imaging can answer this. Generally, candidates have end-stage joint disease where the bone and disc are destroyed or the joint is fused, and where conservative or joint-sparing options are no longer effective.
Is total TMJ joint replacement safe? Total joint replacement is a well-established reconstructive procedure with decades of published outcomes in carefully selected patients. As with any major surgery, it carries risks, which your surgeon will review with you in detail before you decide. Choosing a surgeon with focused experience matters — you can review Dr. Wolford’s background and training when weighing your options.
How long is recovery? Recovery varies by patient and by whether jaw-position surgery is performed at the same time. Your surgeon will give you a personalized timeline for diet progression, jaw physiotherapy, and return to activity at your consultation.
Will insurance cover it? Total TMJ reconstruction is frequently a covered medical procedure when medically necessary. When surgery is recommended, the office prepares a pre-authorization letter for your insurance company. Coverage depends on your individual plan.
Why is the jaw sometimes repositioned during the same surgery? Because TMJ pathology and jaw deformity often occur together. Correcting both in one planned operation can improve stability and reduce overall treatment time compared with treating the joint in isolation.
Can a night guard or physical therapy fix end-stage disease? No. Those manage symptoms and are valuable earlier in the disease, but they cannot restore a joint whose bone and disc have already been destroyed.
About the Author
Larry M. Wolford, DMD is a board-certified oral and maxillofacial surgeon in Dallas, Texas (NPI 1821178955; National Provider Taxonomy: Oral & Maxillofacial Surgery, 1223S0112X). He earned his DMD from Temple University School of Dentistry and completed his residency in Oral and Maxillofacial Surgery at the University of Texas Southwestern Medical School in Dallas.
He is a Diplomate of the American Board of Oral and Maxillofacial Surgery and has served on its Advisory Committee, and a Clinical Professor of Oral and Maxillofacial Surgery and Orthodontics at Texas A&M University Health Science Center, Baylor College of Dentistry. His professional memberships include the American Association of Oral and Maxillofacial Surgeons, the American Society of TMJ Surgeons, the American Academy of Craniomaxillofacial Surgeons, and the American Academy of Craniofacial Pain.
Over a career spanning more than four decades, Dr. Wolford has authored over 185 peer-reviewed publications and more than 150 scientific abstracts, helped develop surgical techniques used internationally (including the Mitek Anchor articular disc repositioning technique), and has performed more patient-fitted total TMJ joint prostheses than any other surgeon in the country. He has trained hundreds of surgeons through fellowship programs and lectures worldwide on orthognathic and TMJ surgery.
Practice: Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 · Free initial telephone consultation: 214-828-9115
Verify credentials via the NPPES NPI Registry.
Related Reading on This Site
- TMJ Dysfunction: Symptoms and Treatment
- Total TMJ Replacement: Comprehensive Clinical Article
- Total TMJ Replacement: A Patient’s Guide to Custom Joint Prosthetics, Recovery, and Outcomes
- Oral and Maxillofacial Surgery
- About Dr. Larry M. Wolford, DMD
- Patient Information
- Contact the Office
Authoritative Resources (External)
These independent, non-commercial sources offer further patient education and oversight information:
- National Institute of Dental and Craniofacial Research (NIH): Temporomandibular Disorders (TMD) overview
- U.S. Food and Drug Administration: Temporomandibular Joint (TMJ) Implants and the FDA’s role in approving and monitoring TMJ implants
- The TMJ Association (nonprofit patient advocacy): Living with TMJ and TMJ implant information
A note on patient stories: Any patient example used in marketing for this practice should be either fully de-identified or used only with written patient authorization, consistent with HIPAA. The scenarios described in this article are general and composite, not specific patients.