Medically reviewed and authored by Larry M. Wolford, DMD — Board-Certified Oral & Maxillofacial Surgeon, Dallas, TX. Last reviewed: May 2026.
Educational disclaimer: This article is for general educational purposes and is not a substitute for an individualized medical evaluation. Diagnosis and treatment of condylar hyperplasia require in-person examination, imaging, and sometimes a bone scan. No outcome is guaranteed; results vary by patient.
Line up a few photos a couple of years apart and the change is hard to unsee: the chin has drifted to one side, one cheek sits lower or fuller than the other, the smile has gone slightly off-level. The bite has shifted too — a crossbite that wasn’t there before, or a gap that won’t close. Often there’s no pain at all. Just a face that is quietly, steadily becoming less symmetrical, and a sense that something is still moving.
That movement is the whole point. When one side of the lower jaw keeps growing after it should have stopped, the asymmetry doesn’t plateau on its own — and the first job is to find out whether the growth is still active.
The Real Problem: An Overactive Jaw Growth Center
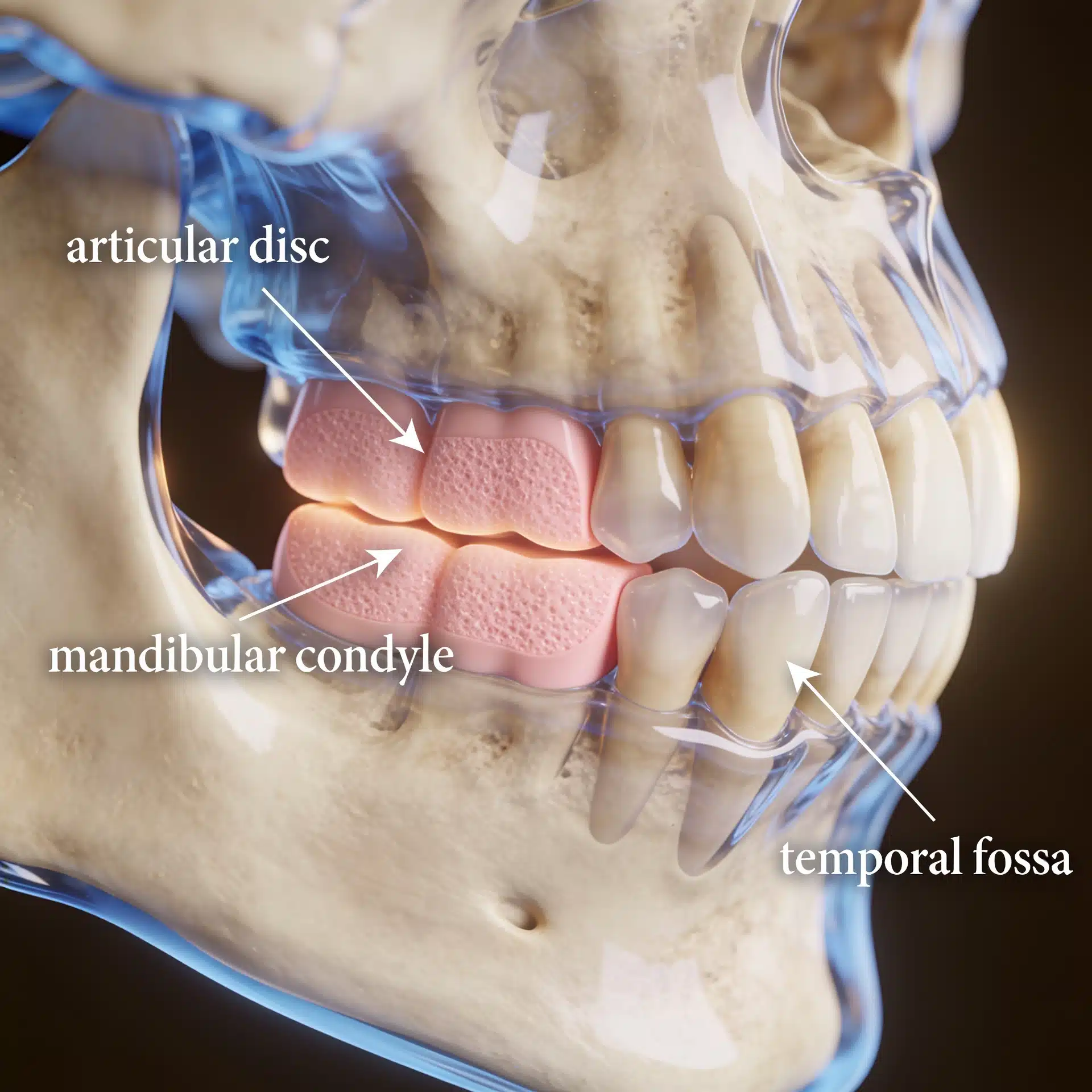
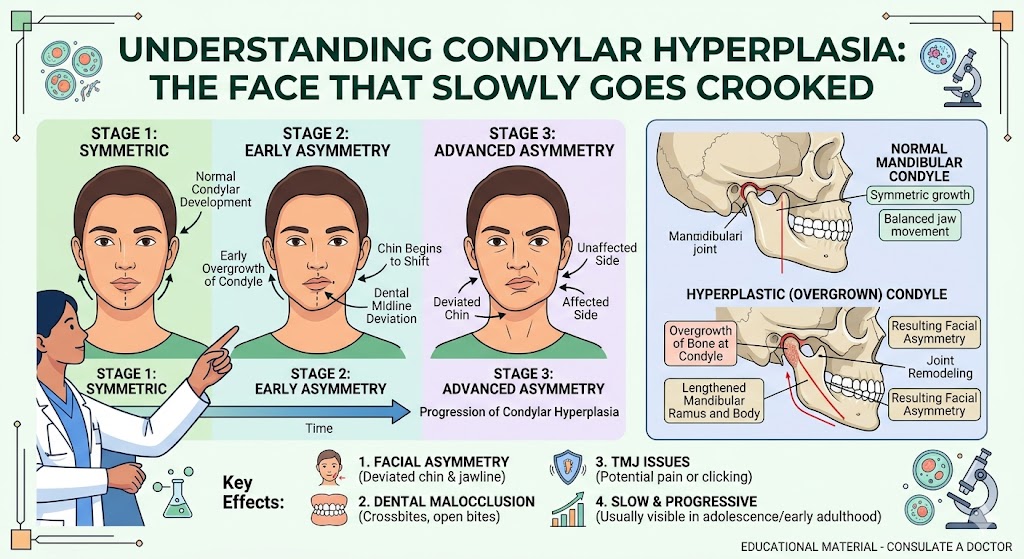
The condyles — the rounded tops of the lower jaw — are the jaw’s growth centers. Condylar hyperplasia is what happens when one (or, less often, both) keeps growing abnormally: too long, too fast, or because of a benign tumor in the growth center. The result is progressive enlargement of the condyle and the jaw, which deviates the chin, cants the bite, and produces facial asymmetry. It typically shows up during the active growth years — adolescence into the mid-twenties — and, apart from appearance and bite changes, is frequently painless.
This is also a condition that is easy to misread as a simple orthodontic problem. A developing crossbite or jaw deviation gets treated as malocclusion, while the underlying engine — an overgrowing condyle — keeps running. The asymmetry is the symptom; the growth center is the cause.
Because “condylar hyperplasia” actually covers several distinct conditions, sorting out which one a patient has matters. Dr. Wolford developed a widely used classification that separates the common form of accelerated condylar growth (which can be bilateral or one-sided) from enlargement caused by an osteochondroma or other tumors, and from rarer malignant causes. Each behaves differently and is treated differently — which is exactly why a precise diagnosis comes before any plan.

What an Experienced Surgeon Brings to the Decision
The value of a focused practice here is distinguishing active growth from finished growth, and identifying the type of hyperplasia before operating — because doing corrective jaw surgery while the condyle is still growing predictably relapses.
Dr. Wolford authored the peer-reviewed classification system for condylar hyperplasia now referenced internationally, and has more than four decades of experience treating facial asymmetry of jaw-growth origin. When indicated, he performs the condylectomy that removes the overactive growth center together with disc repositioning and the corrective jaw surgery needed to rebalance the face — frequently in a single, coordinated operation. He has authored over 185 peer-reviewed publications across his career. That experience doesn’t change your anatomy, but it changes how accurately the cause is identified and how completely it’s addressed. (The practice’s overview of mandibular condylar hyperplasia details the classification and treatment.)
Key Takeaways
- Condylar hyperplasia is abnormal overgrowth of the jaw’s condyle — a growth-center problem, not a simple orthodontic one.
- It causes progressive facial asymmetry, chin deviation, and bite changes, usually during the growth years, and is often painless.
- It isn’t one condition. Accelerated normal growth, osteochondroma, and rarer tumors all enlarge the condyle but behave differently.
- Determining whether growth is still active is decisive — it dictates whether the growth center must be removed.
- Operating on active growth without arresting it tends to relapse. The cause has to be stopped, not just the asymmetry corrected.
- Goals are realistic: halt the abnormal growth, restore facial balance and a functional bite. Outcomes vary and are never guaranteed.
How the Decision Is Actually Made
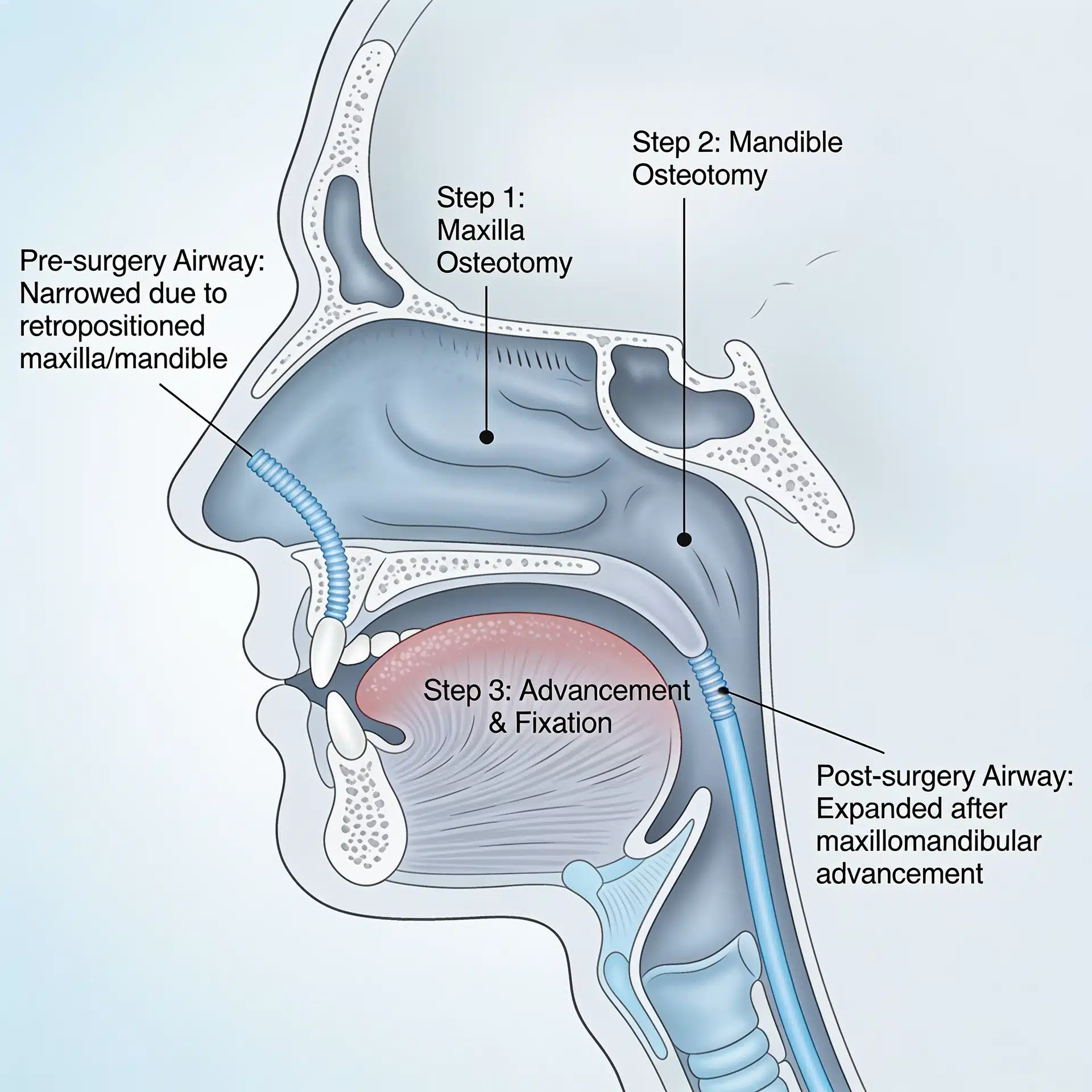
Short answer: Treatment hinges on whether the condyle is still actively growing. If it is, the overactive growth center is removed (condylectomy) to stop progression — often combined with disc repositioning and corrective jaw surgery to rebalance the face. If growth has finished, orthognathic surgery alone may correct the residual asymmetry.
Here is the reasoning behind that answer.
Diagnosis combines serial records, imaging, and sometimes a bone scan. Comparing study models, photos, and radiographs over time helps establish that the asymmetry is progressing. Cone-beam CT maps the bony overgrowth, MRI assesses the joint and disc, and a nuclear bone scan (scintigraphy/SPECT) can help indicate whether the growth center is still metabolically active. (Dr. Wolford’s MRI evaluation overview explains what the joint imaging shows; the National Institutes of Health offers a patient guide to temporomandibular disorders for broader joint context.)
The type of hyperplasia steers the plan. Accelerated growth of an otherwise normal condyle is handled differently from enlargement caused by an osteochondroma, where the tumor itself must be removed. Identifying the type up front prevents under- or over-treating.
Active growth is arrested at the source. When the condyle is still growing, a condylectomy removes the overactive (or tumor-bearing) portion of the condyle to stop the progression. Performed in proportion to the healthy side, it can also begin to correct the deviation directly.
The bite and balance are corrected together when appropriate. In many cases the condylectomy is combined in a single stage with articular disc repositioning (Mitek anchor technique) and corrective jaw surgery — repositioning the jaws and leveling the bite — for a stable, symmetric result. The companion condition, condylar resorption, sits at the opposite end of the same spectrum: one is too much condylar growth, the other too little.
Success is defined honestly. Realistic objectives are to halt the abnormal growth, restore facial symmetry and balance, and establish a functional bite — not a guarantee of perfect symmetry. Every surgery carries risk, and a candid discussion of those risks is part of informed consent.
Where This Care Happens

Dr. Wolford’s practice is located on the campus of Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 — minutes from downtown Dallas and accessible from across the Dallas–Fort Worth metroplex. Valet parking is available, with self-parking in the adjacent building.
Patients and families travel to Dallas from across the country and internationally for evaluation of facial asymmetry, often flying into DFW or Dallas Love Field, because the condition is uncommon and frequently misattributed to ordinary malocclusion. All procedures for both current and new patients are performed exclusively at the Dallas office. Out-of-town patients can review what to bring — including any prior orthodontic records, imaging, and photos over time — on the patient information page. A free initial telephone consultation is available at 214-828-9115, or you can contact the office online.
Frequently Asked Questions
My orthodontist is treating a crossbite. Could it actually be condylar hyperplasia? It can be, especially if the asymmetry is progressing — a chin drifting further off-center, a bite that keeps shifting. Comparison photos over time and proper imaging help tell an active growth problem apart from a stable orthodontic one.
Does condylar hyperplasia hurt? Often not. Many patients have no jaw pain; the main clues are the changing appearance and bite. Absence of pain does not mean the growth has stopped.
How do you know if the jaw is still growing? Through a combination of serial records showing progression and imaging — including, in some cases, a nuclear bone scan that helps indicate whether the growth center is still active. This guides whether the growth center needs to be removed.
Will I need my whole jaw operated on, or just the condyle? It depends on the type and stage. Some patients need only a condylectomy; many benefit from combining it with disc repositioning and corrective jaw surgery in one operation to rebalance the face and bite. Candidacy is individual.
Can it be fixed with braces alone? No. Orthodontics can move teeth but cannot stop an overgrowing condyle or correct the underlying skeletal asymmetry it causes. The growth problem has to be addressed.
What if growth has already stopped? If the hyperplasia is no longer active, the residual asymmetry can often be corrected with orthognathic surgery without removing the condyle.
About the Author
Larry M. Wolford, DMD is a board-certified oral and maxillofacial surgeon in Dallas, Texas (NPI 1821178955; National Provider Taxonomy: Oral & Maxillofacial Surgery, 1223S0112X). He earned his DMD from Temple University School of Dentistry and completed his residency in Oral and Maxillofacial Surgery at the University of Texas Southwestern Medical School in Dallas.
He is a Diplomate of the American Board of Oral and Maxillofacial Surgery and has served on its Advisory Committee, and a Clinical Professor of Oral and Maxillofacial Surgery and Orthodontics at Texas A&M University Health Science Center, Baylor College of Dentistry. His professional memberships include the American Association of Oral and Maxillofacial Surgeons, the American Society of TMJ Surgeons, the American Academy of Craniomaxillofacial Surgeons, and the American Academy of Craniofacial Pain.
Over a career spanning more than four decades, Dr. Wolford has authored over 185 peer-reviewed publications and more than 150 scientific abstracts, holds multiple patents for surgical techniques and devices, and developed a peer-reviewed classification system for condylar hyperplasia that is referenced internationally. He has trained hundreds of surgeons through fellowship programs and lectures worldwide on TMJ and orthognathic surgery.
Practice: Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 · Free initial telephone consultation: 214-828-9115
Verify credentials via the NPPES NPI Registry.
Related Reading on This Site
- Mandibular Condylar Hyperplasia
- Mandibular Condylar Resorption
- MRI Evaluation for TMJ
- Orthognathic Surgery: Correcting Jaw Misalignment
- TMJ Dysfunction: Symptoms and Treatment
- Total TMJ Replacement
- About Dr. Larry M. Wolford, DMD
- Patient Information
- Contact the Office
Authoritative Resources (External)
These independent, non-commercial sources offer further patient education:
- National Institute of Dental and Craniofacial Research (NIH): Temporomandibular Disorders (TMD) overview for general jaw-joint context
- American Association of Oral and Maxillofacial Surgeons (professional society): corrective jaw (orthognathic) surgery overview
- MSD Manual (professional medical reference): mandibular condylar hyperplasia
A note on patient stories: Any patient example used in marketing for this practice should be either fully de-identified or used only with written patient authorization, consistent with HIPAA. Because this condition often affects minors, particular care should be taken with consent and de-identification. The scenarios described in this article are general and composite, not specific patients.