Medically reviewed and authored by Larry M. Wolford, DMD — Board-Certified Oral & Maxillofacial Surgeon, Dallas, TX. Last reviewed: May 2026.
Educational disclaimer: This article is for general educational purposes and is not a substitute for an individualized medical evaluation. Diagnosis and treatment of condylar resorption require in-person examination, imaging, and sometimes laboratory testing. No outcome is guaranteed; results vary by patient.
A teenager’s bite starts to open at the front. Her chin seems to be sliding backward in photos taken a year apart. Braces go on, then come off, then go back on, and the bite keeps drifting open anyway. Sometimes there’s jaw pain or clicking; sometimes there’s nothing at all. Parents are told it’s an overbite, a growth phase, or a compliance problem. Meanwhile, the actual structure of the jaw joint is quietly changing.
This pattern has a name, and recognizing it early matters enormously — because the wrong treatment can make it worse. The condition is idiopathic condylar resorption, and in adolescents it’s often called adolescent internal condylar resorption (AICR).
The Real Problem: A Resorbing Jaw Joint
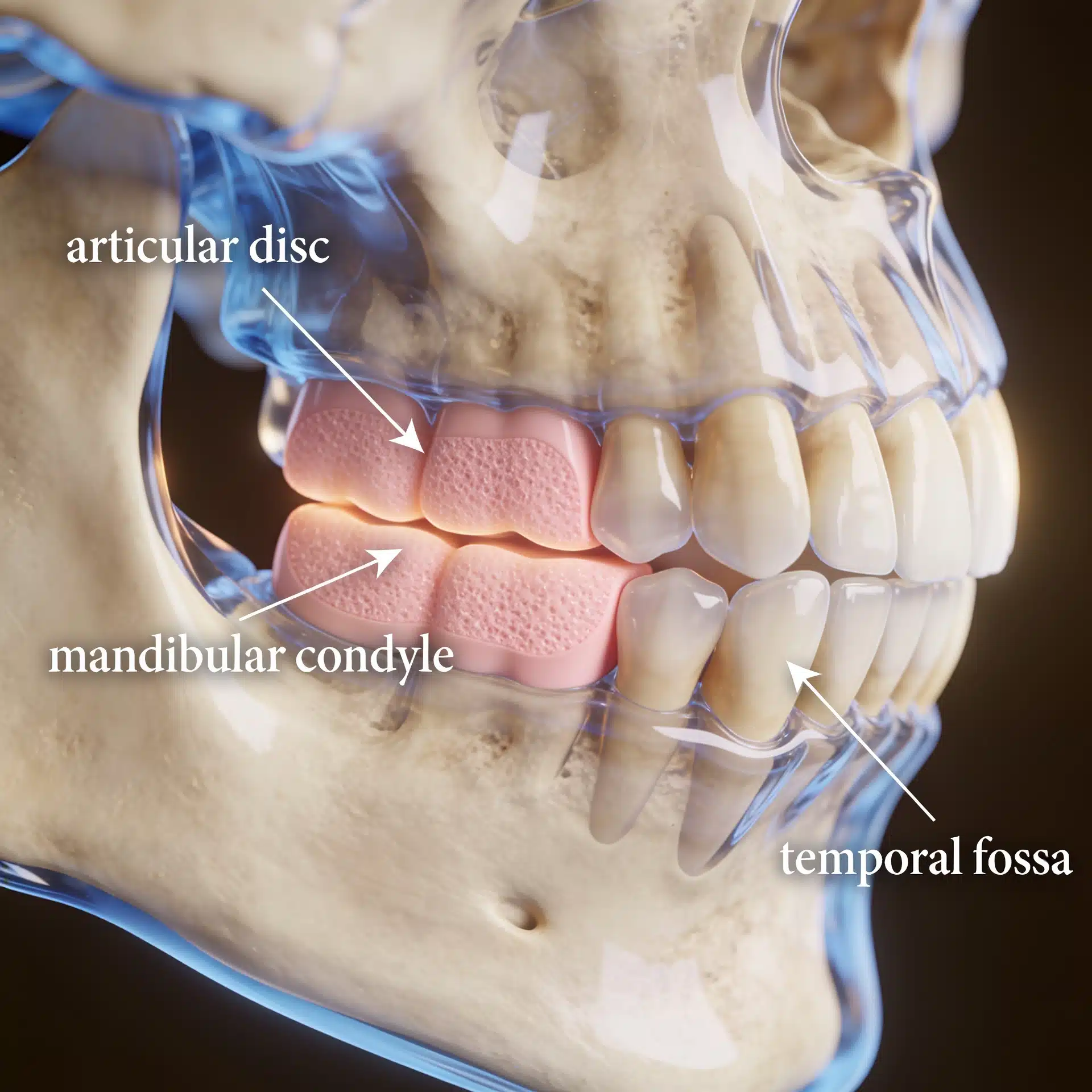
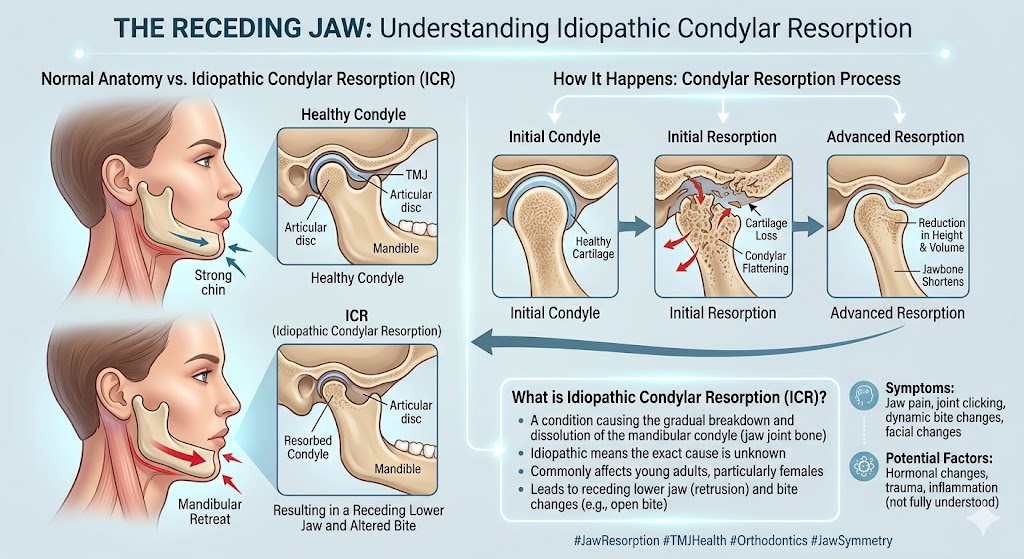
The issue here isn’t orthodontics gone wrong or a cosmetic overbite. It’s a progressive breakdown of bone in the jaw joint. The mandibular condyles — the rounded tops of the lower jaw that fit into the skull — slowly resorb and shrink. As they lose height, the lower jaw rotates backward and down, producing a receding chin, an anterior open bite, and a characteristic steep (high) occlusal-plane facial pattern.
The condition has a striking demographic signature: it appears overwhelmingly in adolescent and young adult females, often beginning during the pubertal growth spurt, and is widely understood to be hormonally influenced. On MRI, the articular discs are typically displaced forward, the condyles look small, and there is non-inflammatory tissue around them. Notably, a meaningful share of patients have no pain at all — which is exactly why the condition is so often missed until the bite and profile have already changed.
Crucially, idiopathic condylar resorption is a diagnosis of exclusion. Other conditions that resorb the condyle — including systemic autoimmune diseases such as rheumatoid arthritis, lupus, scleroderma, and psoriatic arthritis — must be ruled out first. (The National Institute of Arthritis and Musculoskeletal and Skin Diseases provides background on these rheumatic and autoimmune arthritides.) If other joints in the body are involved, the problem may not be idiopathic condylar resorption at all.

What an Experienced TMJ Surgeon Brings to the Decision
The value of a focused practice here is not a promise to reverse what’s lost — it’s recognizing the condition for what it is and choosing a sequence of treatment that doesn’t backfire. This is a diagnosis that general orthodontic and surgical care frequently misreads, and the cost of misreading it is high: treating the bite while ignoring the joint tends to make the resorption worse.
Dr. Wolford has published extensively on adolescent internal condylar resorption, including peer-reviewed work describing its diagnosis and a specific treatment protocol, and has authored over 185 scientific publications across his career. His published studies — and others — have shown that performing orthognathic surgery alone on these patients predictably leads to continued condylar resorption and relapse. That body of work shapes a treatment approach built around the joint, not just the bite. (For the practice’s detailed overview, see Dr. Wolford’s pages on mandibular condylar resorption and adolescent internal condylar resorption.)
Key Takeaways
- Idiopathic condylar resorption is bone breakdown in the jaw joint — not a simple orthodontic overbite.
- It mostly affects adolescent and young adult females and is believed to be hormonally influenced.
- The hallmark signs are a progressively receding chin, a developing anterior open bite, and a steep occlusal-plane facial pattern — sometimes without any pain.
- It is a diagnosis of exclusion. Systemic autoimmune arthritis and other causes must be ruled out first.
- Treating the bite alone tends to fail. Orthognathic surgery without addressing the joint predictably leads to continued resorption and relapse.
- The goal is to stop the disease process first, then correct the bite and jaw position for a stable result. Outcomes vary and are not guaranteed.
How the Decision Is Actually Made
Short answer: Treatment is built around halting the resorption before — or at the same time as — correcting the jaw and bite, because correcting the bite on a joint that is still breaking down predictably relapses.
Here is the reasoning behind that answer.
The diagnosis combines history, imaging, and exclusion. Evaluation typically includes a clinical exam, cone-beam CT of the bones, and an MRI of the joints to assess the discs and condyles. Because idiopathic condylar resorption is diagnosed only after other causes are excluded, lab work may be ordered to screen for systemic autoimmune disease. (For background on the broader category of jaw-joint disorders, see the National Institutes of Health’s guide to temporomandibular disorders and Dr. Wolford’s TMJ dysfunction overview.)
Why bite-only treatment backfires. When the condyles are actively resorbing, moving the jaws into a corrected position doesn’t last — the foundation keeps shrinking underneath. Orthodontics or orthognathic surgery performed without addressing the joint can be followed by renewed resorption, a returning open bite, and worsening symptoms.
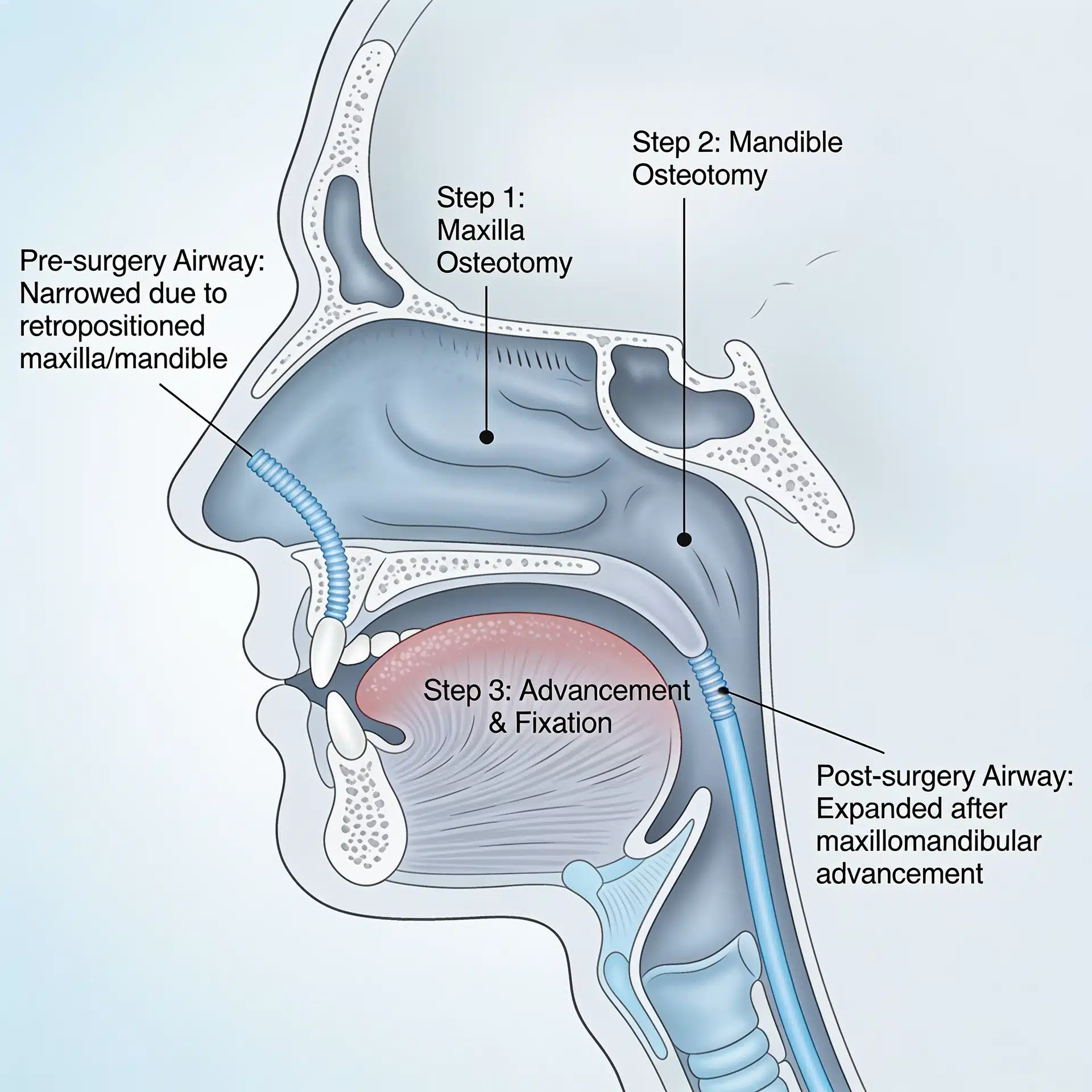
The joint is addressed directly. Depending on the stage, treatment may involve repositioning and stabilizing the displaced articular disc (using the Mitek anchor technique) together with the corrective jaw surgery needed for function and facial balance. In advanced cases where the discs and condyles are no longer salvageable, total TMJ replacement with fat grafting may be used to reconstruct the joints while advancing the jaws — often with counter-clockwise rotation to restore the profile and airway.
Timing and growth matter. In a still-growing adolescent, the activity of the resorption and the patient’s growth status influence when and how to intervene. This is individualized, not formulaic.
Success is defined honestly. Realistic objectives are to stop the active resorption, establish a stable bite, relieve symptoms, and restore facial balance — not to regrow what has already been lost. Every surgery carries risk, and a candid discussion of risks and expectations is part of informed consent. (Understanding the condition is also part of why corrective jaw surgery sometimes needs revision when an underlying joint problem went unrecognized.)
Where This Care Happens

Dr. Wolford’s practice is located on the campus of Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 — minutes from downtown Dallas and accessible from across the Dallas–Fort Worth metroplex. Valet parking is available, with self-parking in the adjacent building.
Families travel to Dallas from across the country and internationally for evaluation of condylar resorption, because the condition is uncommon and frequently misdiagnosed. All procedures for both current and new patients are performed exclusively at the Dallas office. Parents and patients can review what records and imaging to gather — including any prior orthodontic records and photos over time — on the patient information page. A free initial telephone consultation is available at 214-828-9115, or you can contact the office online.
Frequently Asked Questions
My orthodontist says it’s just an overbite. How would I know it’s something more? Warning signs include a chin that recedes over time, a front bite that progressively opens, and a steepening facial profile — especially in an adolescent or young adult female. Comparison photos over months and proper imaging help distinguish ongoing resorption from a stable orthodontic issue.
Does condylar resorption always hurt? No. A significant portion of patients have no jaw pain or joint noise even while the condyles are resorbing. The absence of pain does not mean the joint is healthy.
Is this caused by hormones? The condition is widely understood to be hormonally influenced, which is part of why it clusters in teenage girls and young women. The exact mechanism is still being studied.
Can braces or jaw surgery fix it? Not on their own. Treating the bite while the joint is still resorbing tends to relapse. The joint problem has to be addressed as part of the plan for the result to be stable.
Will my child need a joint replacement? Not necessarily. Earlier-stage disease may be managed by stabilizing the disc along with corrective jaw surgery. Joint replacement is reserved for advanced cases where the discs and condyles can’t be saved. Candidacy is individual.
Why does ruling out other diseases matter? Because systemic autoimmune conditions can resorb the condyle too, and they require different management. A correct diagnosis depends on excluding those causes first.
About the Author
Larry M. Wolford, DMD is a board-certified oral and maxillofacial surgeon in Dallas, Texas (NPI 1821178955; National Provider Taxonomy: Oral & Maxillofacial Surgery, 1223S0112X). He earned his DMD from Temple University School of Dentistry and completed his residency in Oral and Maxillofacial Surgery at the University of Texas Southwestern Medical School in Dallas.
He is a Diplomate of the American Board of Oral and Maxillofacial Surgery and has served on its Advisory Committee, and a Clinical Professor of Oral and Maxillofacial Surgery and Orthodontics at Texas A&M University Health Science Center, Baylor College of Dentistry. His professional memberships include the American Association of Oral and Maxillofacial Surgeons, the American Society of TMJ Surgeons, the American Academy of Craniomaxillofacial Surgeons, and the American Academy of Craniofacial Pain.
Over a career spanning more than four decades, Dr. Wolford has authored over 185 peer-reviewed publications and more than 150 scientific abstracts, holds multiple patents for surgical techniques and devices, and has published widely on temporomandibular joint pathology — including adolescent internal condylar resorption and its diagnosis and treatment. He has trained hundreds of surgeons through fellowship programs and lectures worldwide on TMJ and orthognathic surgery.
Practice: Baylor University Medical Center, Worth Street Tower, 3409 Worth Street, Suite 400, Dallas, TX 75246 · Free initial telephone consultation: 214-828-9115
Verify credentials via the NPPES NPI Registry.
Related Reading on This Site
- Mandibular Condylar Resorption
- Adolescent Internal Condylar Resorption (AICR)
- TMJ Dysfunction: Symptoms and Treatment
- Total TMJ Replacement
- Orthognathic Surgery: Correcting Jaw Misalignment
- About Dr. Larry M. Wolford, DMD
- Patient Information
- Contact the Office
Authoritative Resources (External)
These independent, non-commercial sources offer further patient education:
- National Institute of Dental and Craniofacial Research (NIH): Temporomandibular Disorders (TMD) overview
- National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIH): arthritis and rheumatic diseases overview and rheumatoid arthritis (relevant to ruling out systemic causes)
A note on patient stories: Any patient example used in marketing for this practice should be either fully de-identified or used only with written patient authorization, consistent with HIPAA. Because this condition commonly affects minors, particular care should be taken with consent and de-identification. The scenarios described in this article are general and composite, not specific patients.