Every time you speak, chew, or yawn, a small but remarkably complex joint makes it possible. The temporomandibular joint (TMJ) connects the lower jaw — the mandible — to the temporal bone of the skull, one on each side of the face. Acting as a hinge and a sliding joint simultaneously, it is one of the most frequently used joints in the human body. When it functions well, you never think about it. When it doesn’t, the consequences can be difficult to ignore.
Temporomandibular disorders (TMDs) are a group of more than 30 conditions that cause pain and dysfunction in the jaw joint and the muscles that control jaw movement. According to the National Institute of Dental and Craniofacial Research (NIDCR), approximately 11 to 12 million adults in the United States experience pain in the temporomandibular joint region — and the condition is twice as common in women as in men, particularly among women aged 35 to 44.
This guide covers everything you need to know about TMJ disorders: what causes them, how to recognize the symptoms, and what treatment options — both conservative and surgical — are available to you.
What Is the TMJ and Why Does It Matter?
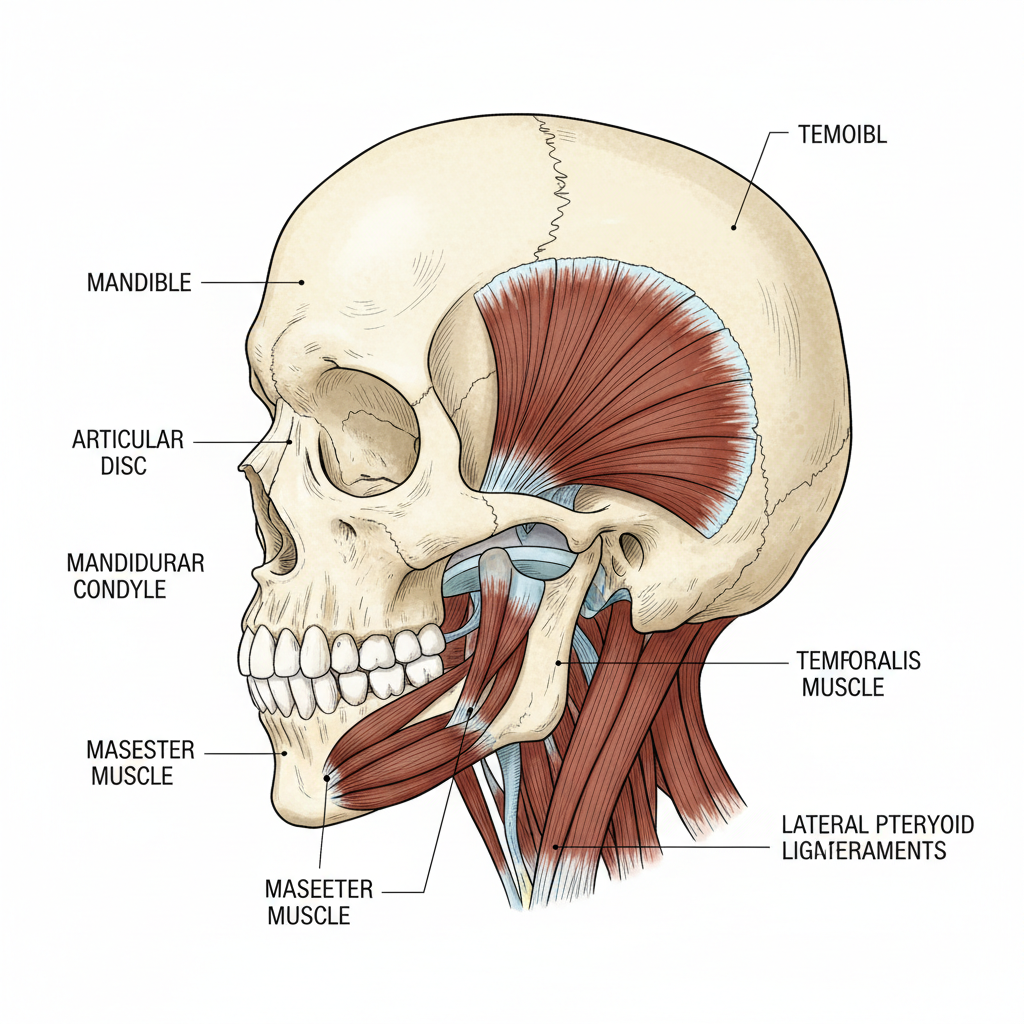
The temporomandibular joint is unique in the body. Unlike a pure hinge joint, it combines rotational and translational movement, allowing the jaw to open, close, shift side to side, and protrude forward. A small disc of cartilage sits between the condyle (the rounded end of the lower jaw) and the temporal bone, acting as a cushion and keeping movement smooth.
Supporting this joint is a network of muscles, ligaments, and tendons — all of which must work in coordination for normal jaw function. Disruption to any one of these structures can produce pain, dysfunction, or both.
What Causes TMJ Disorders?
The causes of TMDs are often multifactorial. In many cases, no single identifiable trigger exists. The NIDCR notes that current research points to a combination of genetic predisposition, psychological stressors, and individual differences in pain perception as contributing factors.
That said, several specific conditions are consistently associated with TMJ disorders:
- Arthritis: Both osteoarthritis and rheumatoid arthritis can affect the temporomandibular joint. Osteoarthritis involves the gradual breakdown of cartilage within the joint, while rheumatoid arthritis triggers an inflammatory autoimmune response that can damage joint tissue.
- Jaw or joint injury: Trauma — such as a blow to the jaw, whiplash, or a fracture — can damage the condyle, the articular disc, or the surrounding structures, leading to acute or chronic TMJ symptoms.
- Disc displacement: The articular disc can shift out of its normal position, either reducing (clicking in and out) or becoming permanently displaced. This is one of the most frequently diagnosed intra-articular conditions. The American Association of Oral and Maxillofacial Surgeons (AAOMS) emphasizes that symptomatic disc displacement should only be considered causative after synovitis and capsular impingement have been addressed.
- Synovitis: Inflammation of the synovial membrane lining the joint can generate pain, edema, and restricted movement. This is now understood to be a primary driver of intra-articular pain and dysfunction, triggering a cascade of molecular events that, if left untreated, can lead to cartilage and bone damage.
- Bruxism and parafunctional habits: Chronic teeth clenching or grinding places excessive mechanical load on the joint, increasing the risk of inflammatory responses and tissue damage over time.
- Structural or developmental abnormalities: Conditions present from birth or that develop during growth — such as condylar hyperplasia or hypoplasia — can alter the biomechanics of the joint and contribute to pain and asymmetry.
Notably, the NIDCR confirms that research does not support the long-held belief that a misaligned bite or orthodontic braces directly cause TMDs.
Recognizing the Symptoms of TMJ Disorders
TMJ symptoms vary widely between individuals, ranging from mild and intermittent to severe and debilitating. It is important to note that clicking or popping sounds in the jaw without pain are common and considered normal — they do not require treatment on their own.
However, the following symptoms may indicate a TMD and warrant evaluation by a qualified specialist:
- Jaw or facial pain — the most frequently reported symptom, often felt in the joint itself or in the surrounding muscles
- Pain that spreads to the neck or face
- Jaw stiffness, especially upon waking
- Limited range of motion, including difficulty fully opening the mouth
- Jaw locking — the jaw becoming stuck in an open or closed position
- Painful clicking, popping, or grating during jaw movement
- Earache, tinnitus (ringing in the ears), hearing changes, or dizziness
- A change in how the upper and lower teeth fit together (bite shift)
TMDs can also co-occur with other pain conditions, including headaches, back pain, fibromyalgia, and sleep disorders. Identifying the full clinical picture is essential to accurate diagnosis and effective treatment planning.
Diagnosing TMJ Disorders
There is currently no single universally accepted diagnostic test for TMDs. Diagnosis relies on a thorough clinical history, a detailed physical examination, and, where appropriate, advanced imaging.
According to the Mayo Clinic, a clinician will typically:
- Palpate the jaw and surrounding muscles to identify areas of tenderness
- Assess range of motion and jaw movement patterns
- Listen for joint sounds with the aid of a stethoscope
Imaging studies — including panoramic X-rays, cone-beam CT (CBCT), medical-grade CT scans, and MRI — are often recommended to assess bone structure, disc position, and soft tissue changes. The AAOMS position paper notes that MRI remains the standard for evaluating soft tissue, while CT imaging is preferred for diagnosing osseous changes such as osteoarthritis.
In complex cases, TMJ arthroscopy may be used diagnostically to directly visualize the joint interior and guide subsequent treatment decisions.
Treatment Options for TMJ Disorders
The treatment of TMDs follows a clear clinical principle: begin with the least invasive approach and escalate only when necessary. Most cases of TMD respond well to conservative, non-surgical management — and many resolve without any formal treatment at all.
Conservative and Non-Surgical Treatments
Self-management is frequently the appropriate first step. The NIDCR recommends:
- Eating soft foods and avoiding hard, chewy, or sticky items
- Applying heat or ice to the affected area
- Reducing habits that stress the jaw, such as clenching, nail biting, or gum chewing
- Taking over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen
Physical therapy plays a meaningful role in TMD management. Manual therapy — where a trained therapist works to stretch and mobilize soft tissues around the joint — has demonstrated effectiveness in improving function and reducing pain.
Behavioral health approaches, including cognitive behavioral therapy (CBT) and biofeedback, have also shown clinical benefit. CBT addresses the thought patterns and stress responses that can amplify pain perception, while biofeedback teaches patients to recognize and relax jaw muscle tension in real time.
Intraoral appliances (also called splints, nightguards, or occlusal appliances) are commonly prescribed. They do not alter the bite or teeth permanently, and evidence suggests they may provide symptom relief in some patients — though the precise mechanism remains a subject of ongoing research.
Medications — including prescription NSAIDs, muscle relaxants, tricyclic antidepressants, and antianxiety agents — may be recommended as part of a comprehensive management plan.
For complementary approaches, both acupuncture and transcutaneous electrical nerve stimulation (TENS) have been studied in the context of TMDs, with some patients reporting benefit. More information on relaxation and complementary techniques is available through the National Center for Complementary and Integrative Health (NCCIH).
Minimally Invasive Surgical Procedures
When conservative treatments fail to provide adequate relief, minimally invasive procedures are the next appropriate consideration.
Arthrocentesis involves inserting small needles into the joint space to flush it with fluid, removing inflammatory mediators, degraded proteins, and adhesions. The AAOMS reports pain relief and improved range of motion in 70 to 95 percent of patients treated with arthrocentesis.
Arthroscopy takes this a step further, allowing the surgeon to directly visualize the joint interior and address specific pathology — including synovial plica, fibrous adhesions, capsular impingement, and chondromalacia. Reported outcomes show pain reduction and improved function in 80 to 90 percent of patients, and comparative studies suggest arthroscopy is superior to arthrocentesis in outcome measures.
Open Joint Surgery and Total Joint Replacement
For patients with severe, refractory TMJ disease — including advanced osteoarthritis, joint ankylosis (fusion), prior failed surgery, or significant structural damage — open joint surgery or total joint replacement (TJR) may be the most appropriate course of action.
Total joint replacement involves replacing the entire joint with a custom-fitted or stock alloplastic prosthesis. According to the AAOMS, TJR is especially indicated when osteoarthritis is confirmed on CT imaging, as all pathologically involved tissues can be removed. Studies on long-term outcomes of custom-fitted total TMJ prostheses have demonstrated significantly reduced pain, improved jaw function, and the ability to eat solid food in appropriately selected patients.
Dr. Larry M. Wolford — an internationally recognized oral and maxillofacial surgeon and researcher — is among the most published and cited authorities in the field of TMJ surgery. Dr. Wolford has contributed extensively to the clinical literature, including peer-reviewed research on disc repositioning techniques using the Mitek mini anchor and on the management of infected TMJ total joint prostheses. His work, published in the Journal of Oral and Maxillofacial Surgery and other leading medical journals, has influenced surgical protocols adopted by surgeons around the world.
Surgical approaches to the TMJ are complex and carry inherent risks, including permanent changes to joint anatomy. As such, the NIDCR and AAOMS strongly recommend obtaining multiple specialist opinions before proceeding with any irreversible intervention, and seeking care from a surgeon who specializes in TMJ disorders when open joint surgery or TJR is being considered.
The Importance of Early Diagnosis and Specialized Care
The path from early-stage TMJ discomfort to complex joint pathology is not inevitable. Many patients who act early — with appropriate conservative management — achieve substantial relief and avoid surgical intervention altogether. However, for those with progressive joint disease, delayed diagnosis can allow synovitis and structural deterioration to advance to a point where more extensive treatment becomes necessary.
Seeking evaluation from a qualified specialist is the most important step any patient can take. The TMJ Association, a nonprofit patient advocacy organization, provides resources to help patients understand their diagnosis and navigate treatment decisions. For foundational clinical information, the NIDCR and MedlinePlus offer peer-reviewed, regularly updated guidance.
Take Control of Your TMJ Health
TMJ disorders are real, complex, and — in many cases — highly treatable. Understanding the anatomy involved, recognizing the warning signs, and acting on them promptly can make a meaningful difference in outcomes. From self-care strategies and physical therapy to advanced surgical reconstruction, the spectrum of available treatments continues to evolve with the science.
If you are experiencing jaw pain, restricted movement, or other symptoms consistent with a TMJ disorder, consult a qualified dental or medical professional. For cases requiring surgical expertise, specialized care from a surgeon with advanced training and a documented record in TMJ surgery is not just advisable — it is essential.









